Kim Potter Guilty. Like Confusing Bacon w/Eggs: White Jury Didn't Believe Cop-Actress Made a Mistake When She Fatally Shot Black Man, Rejecting her White Skin Defense in Random Surprise Justice
/
From [HERE] Kimberly Potter, the former Brooklyn Center, Minn., police officer who shot and killed Daunte Wright during a traffic stop in April, was found guilty of first- and second-degree manslaughter by a Hennepin County jury on Thursday. The jury was mostly white.
Ms. Potter, a 26-year veteran of the force, testified that she thought she had drawn her stun gun when she shot the 20-year-old in the chest with her 9mm handgun. She betrayed little emotion as the verdict was read.
The jury had deliberated for around 28 hours over four days, following nine days of testimony and arguments.
Ms. Potter could face up to 15 years in prison for first-degree manslaughter and up to 10 years in prison for second-degree manslaughter. On the first-degree count, the jury found Ms. Potter guilty of taking a life while committing another crime, in this case, the reckless handling of a firearm. The second-degree verdict represented the jury finding Ms. Potter culpably negligent for the killing.
Defense lawyers said they planned to argue for a reduced sentence, citing Ms. Potter’s long record of public service and lack of prior charges. They also asked the judge to allow her to remain on bail ahead of sentencing.
“She’s not going to run, she’s obviously not going to commit any more crimes,” lawyer Earl Gray told the judge shortly after the verdict. “She’s been convicted of an accident.”
Judge Regina Chu said she couldn’t handle Ms. Potter’s case differently than any other and ordered her into custody pending sentencing, which was set for Feb. 18. Ms. Potter had been free on $100,000 in bail.
Minnesota Attorney General Keith Ellison, whose office prosecuted the case, thanked the jury and noted that the verdict wouldn’t restore Mr. Wright’s life, but it did represent a degree of accountability. “Accountability is an important step, a critical, necessary step on the road to justice for us all,” he said.
In closing arguments on Monday, prosecutors argued that Ms. Potter should be found guilty for her reckless actions. “What this case is really about is about an officer who mishandled her firearm,” said prosecutor Erin Eldridge, an assistant attorney general for the state of Minnesota. She urged jurors not to speculate or “get sucked down into that rabbit hole of hypotheticals and misdirection.”
According to the criminal complaint
On April 11, 2021, around 1:53 p.m., Brooklyn Center Police Officer Anthony Luckey and his Field Training Officer, Defendant KIMBERLY ANN POTTER (DOB: 06/18/1972) conducted a traffic stop on a white Buick bearing Minnesota license plate 841UBY near 63rd Avenue North and Orchard Avenue North in Brooklyn Center, Hennepin County, Minnesota. Officer Luckey identified the driver as Daunte Demetrius Wright. There was also an adult female passenger in the front passenger seat. Officer Luckey informed Mr. Wright that the officers stopped him because the vehicle had an air freshener hanging from the rearview mirror and the tabs on the Buick were expired. Officer Luckey returned to his squad car to conduct a record check for Mr. Wright, during which he learned that Mr. Wright had an outstanding arrest warrant for a gross misdemeanor weapons violation. As Officer Luckey ran these checks, Sergeant Mychal Johnson arrived to assist the officers. Officer Luckey and Defendant then re-approached the driver’s side of the Buick to arrest Mr. Wright on the warrant. Sergeant Johnson approached the passenger side of the vehicle.
According to time stamped BWC footage, at 2:01:11 p.m., Officer Luckey asked Mr. Wright to step out of the vehicle. Mr. Wright opened the door of the Buick at 2:01:22 p.m. and got out of the Buick at 2:01:30 p.m. At 2:01:31, Officer Luckey asked Mr. Wright to turn around and place his hands behind his back. Mr. Wright did so. Officer Luckey then began attempting to handcuff Mr. Wright. At 2:01:36 p.m., Sergeant Johnson told Mr. Wright that he was under arrest and at 2:01:39 p.m., Defendant added that Mr. Wright had a warrant.
At 2:01:43 p.m., Officer Luckey told Mr. Wright not to tense up. At that time, Officer Luckey and Mr. Wright were standing near the open driver’s side door of the Buick. Defendant was standing behind and to the right of Officer Luckey. Defendant walked up to Mr. Wright at 2:01:45 p.m. and, at 2:01:48 p.m., took a piece of paper from Mr. Wright’s hand using her left hand. Defendant immediately transferred the paper to her right hand. At 2:01:49 p.m., Mr. Wright pulled away from Officer Luckey and got back into the driver’s compartment of the Buick. Officer Luckey maintained a grip on Mr. Wright, to keep physical control of him so as to pull Mr. Wright back out of the Buick. Sergeant Johnson, who was on the other side of the vehicle, leaned inside the Buick through the passenger door.
At 2:01:55 p.m., Defendant stated, “I’ll tase ya,” and simultaneously moved the piece of paper she was holding from her right hand to her left hand. One second later, at 2:01:56 p.m., Defendant’s right hand, holding her department-issued Glock 9mm handgun, came into view of her BWC. Defendant pointed her handgun at Mr. Wright and tracked with Mr. Wright’s movements as he and Officer Luckey continued moving. Defendant again announced, “I’ll tase you,” at 2:01:58 p.m. and continued pointing her handgun at Mr. Wright.
At 2:02:00 p.m., Defendant said, “Taser, Taser, Taser.” Sergeant Johnson and Officer Luckey both immediately began disengaging from Mr. Wright. One second later, at 02:02:01 p.m., Defendant pulled the trigger and discharged her handgun one time, firing a single round of ammunition. The bullet entered the left side of Mr. Wright’s chest and sequentially perforated the left 6th rib and 5th intercostal muscles, left lung, pericardium, heart, pericardium once again, right lung, and right 4th intercostal muscles before partially exiting the right chest wall, perforating the skin, and becoming lodged in the right side of Mr. Wright’s chest. When she fired the handgun, Defendant was standing outside the driver’s side door and in close proximity to Officer Luckey. Defendant’s handgun was just inches below Officer Luckey’s arm pointing into the driver’s compartment of the Buick, in the direction of Mr. Wright, the passenger, and Sergeant Johnson. Defendant fired her handgun close to Officer Luckey’s face, and the discharged cartridge casing from Defendant’s handgun appeared to strike Officer Luckey in the face as it was ejected. At 2:02:02 p.m., Mr. Wright said, “Ah, he shot me.” The Buick then traveled short distance down the street, where it crashed into another vehicle. Defendant stated at 2:02:03 p.m., “Shit!” and at 2:02:05 p.m., “I just shot him.” Another officer asked, “you did?” and Defendant responded, “yes.” At 2:02:09 p.m., Defendant stated, “I grabbed the wrong fucking gun,” and repeated again, “I shot him.” At 2:03:09 p.m., Defendant stated, “I’m going to go to prison.” At 2:07:27, Defendant stated, “I killed a boy.” Other officers and paramedics responded. Medical personnel were unable to revive Mr. Wright and Mr. Wright was pronounced dead on scene at 2:18 p.m. Assistant Hennepin County Medical Examiner Dr. Lorren Jackson later conducted an autopsy and determined Mr. Wright’s cause of death to be a gunshot wound and deemed the manner of death a homicide.

Dr. Mercola Estimates that More Adults and Kids Have Died From COVID Injections than the Virus based on CDC's Acknowledgment that VAERS Undercounts the Number of Vax Deaths (reporting only 1%)
/STORY AT-A-GLANCE
One team published an engineering analysis to determine the current underreporting factor (URF) from the VAERS information and found the factor to be 41. When applied against the government data they found 173% more children died from the vaccine than from the illness
Using this same URF, the number of deaths from COVID rose to 815,326 and the number permanently disabled to 1,338,404. To date, the total reported deaths from the infection is 803,043, which means the shot has killed more children and adults than the virus
Although there is little reason to give children the shot, officials are spinning the idea that it is needed for herd immunity. Yet, health officials must be aware there is a significant lack of evidence to support this, and children are dying in the process
Pilot deaths and injuries affect commercial flights, logistical distribution of goods and military readiness. In one affidavit as part of a federal lawsuit against the military vaccine mandate, physician Lt. Col. Theresa Long alleges protocols are not followed after the COVID shot

From [Mercola] and [HERE] Many scientists and health experts have warned that vaccinating children against COVID-19 is unnecessary and extremely risky. Since the beginning of the pandemic, it has been obvious that children were at exceptionally low risk for hospitalization and death from the infection.1 Despite this, massive efforts are underway to ensure that every child gets a shot.
If the current data from the Vaccine Adverse Events Reporting System (VAERS)2 are any indication of what the future holds, we are facing the greatest public health calamity in modern history. I believe it is not a new COVID-19 variant causing this, but the current vaccination campaign. Unfortunately, I have no doubt that the deaths caused by the vaccines will end up far exceeding the number of deaths from the illness.
Despite the clear and present dangers of this genetic therapy, vaccine makers, encouraged and endorsed by government health agencies, are steamrolling ahead with trials and recommendations for the shot in children. In May 2021 parents found out that their children can get vaccinated without their consent if they fall under something called the “mature minor” doctrine. 3
This allows providers to treat minors, without parental consent, under certain circumstances. The age group under question was between ages 14 and 18 when there is a “rebuttable presumption of capacity, and the physician may treat without parental consent unless the physician believes that the minor is not sufficiently mature to make his or her own health care decisions.”
In July, two lawsuits were filed in federal court that challenged the Washington D.C. city law which allowed minors to be vaccinated without parental consent.4 In September 2021, The Guardian reported that children aged 12 to 15 in the U.K. may be administered a COVID-19 shot by teams in the school system without parental consent.5
If parents do not consent but the child wants the vaccine, the team can determine if a 12-year-old is able to make an informed decision. Most recently, one California mother spoke to the news media and expressed outrage after the school system allegedly offered her son a pizza in exchange for his taking the genetic therapy shot.6
With each passing month, it becomes more obvious that the battleground in the fight for liberty and freedom has been taken to our young children. A recent review of data7 from the CDC and the Vaccine Adverse Event Reporting System (VAERS) shows that more children have died from the vaccine than have died from the illness.
VAERS Underreporting Factor Affects Data
To compare the number of deaths from COVID illness against those who have died from the genetic therapy injection, we must address the known underreporting factor in VAERS. To date, the VAERS database is the only reporting system used by the CDC and FDA that is accessible to the public. According to VAERS, it:8
“… is a passive reporting system, meaning it relies on individuals to send in reports of their experiences. Anyone can submit a report to VAERS, including parents and patients.”
Additionally, it is the only area where the public, including doctors and other medical professionals, can voluntarily report vaccine adverse events, including death. According to VAERS,9 health care professionals are mandated by law to report serious injury adverse events that occur within a specified time period after the shot, and those events that are listed by the manufacturer as a contraindication to further doses.
However, the system only “encourages” providers to report events after vaccination whether the shot caused the event or not. In other words, the system depends on the health care professionals' knowledge that the VAERS system exists and their willingness to spend time filling out the document which asks for:10
While much of this information is necessary for data tracking, you can see how the time-consuming nature of filling out this form can easily become overwhelming when doctors have multiple patients with adverse events from the COVID-19 shots.11 Lack of knowledge of the system, and a growing physician shortage12 with subsequent lack of time have also likely contributed to the underreporting factor (URF).
In an early grant report submitted by the U.S. Department of Health and Human Services, which is part of the VAERS system, the writers admitted that:13
“Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.”
As of December 3, 2021, there were 946,461 adverse events and 19,886 deaths reported to the system.14 If only 1% of the events are reported, this translates to 94.64 million adverse events and 1.98 million deaths. To ascertain a better estimate of how many people have been injured from the current genetic injection, the issue of the URF was again addressed in a paper published in November 2021.15
The process for defining a new URF was published in a 62-page paper.16 Using an engineering analysis of the available data and judgment based on peer reviewed literature and expertise of the scientists, an underreporting factor of 41 was determined.
Agency Data Show 173% More Children Died From Shot Than Virus
In this short video, you’ll hear just several of the stories of parents who are grieving the loss of their children after giving them a vaccine they were promised would protect them. Many, thinking they were doing the right thing, took an experimental shot and have left devastated parents and families behind.
While evaluating the data, one of the writers of the paper, Steve Kirsch, recognized the gravity of the situation as it relates to the number of children who have died after taking the vaccine versus the number who have died from the illness. CDC data ending December 8, 2021,17 shows 757 children younger than 18 were listed as casualties of COVID-19.
He points out that many of these deaths, like those in adults, are likely children who died with COVID and not from COVID.18 However, to maintain simplicity, he used those numbers for comparison. Then, using data from VAERS ending December 3, 2021, he found 32 deaths from the vaccine.
Using the URF of 41, this suggests there have been 1,312 deaths that are likely to have been caused by the injection as compared to the 757 deaths the CDC records as having been caused by the illness. If you do the math, this means the shot has killed roughly 173% more children than the illness.
Using the same URF of 41 and the current data ending December 3, 2021, from OpenVAERS we can estimate there should have been 38,804,901 reports and 815,326 deaths caused by the injection. This is vitally important as the total number of deaths recorded for COVID-19 as of December 15, 2021. is 795,839.19 This means the shot has currently killed more children and adults than the virus.
Pilot Deaths, Injuries and Shot Mandates Affect Shortage
Pilot deaths and injuries affect commercial flights, logistical distribution of goods and military readiness. In mid-2020, thousands of pilots were laid off or decided to retire when flights were canceled around the country and around the world during lockdowns. Government mandates for the genetic therapy shot have also curbed the hiring of potential aviators.21
It takes up to two years to train a pilot, and Boeing estimates there will be a need for more than 600,000 new pilots over the next two decades. After the release of the shot in 2021, some noted an excessive number of pilot deaths in 2021, versus the number who died in 2019 and 2020.22
As the data on this situation continue to be released, it’s important to note that one Army flight surgeon has also stepped forward to warn that the COVID jab may increase the risk of sudden cardiac death among military pilots.23
Physician Lt. Col. Theresa Long filed an affidavit alleging the Army isn’t following DOD protocols to screen for side effects of myocarditis associated with the Pfizer and Moderna shots. The affidavit is part of a federal lawsuit against the vaccine mandate for the U.S. military. In the affidavit Long claims:24
“… there is no functional myocardial screening currently being conducted … it is my professional opinion that substantial foreseen risks currently exist, which require proper screening of all flight crews. Based on the DOD’s own protocols and studies, the only two valuable methodologies to adequately assess this risk are through MRI imaging or cardio biopsy which must be carried-out.”
In October 2021, The Defender,25 the publication of the Children’s Health Defense, asked a question that many may have overlooked. Are these vaccine mandates that appear to be reducing critical services and personnel, such as pilots, health care providers and first responders, an intentional sabotage designed to weaken America and expand control?
The loss of critical pilots is not only the result of death, but also life-altering disabilities after the shot. The Defender26 covered Sen. Ron Johnson’s, R-Wis., expert panel on COVID vaccine injuries, during which a 33-year-old commercial airline pilot from Cleveland, Mississippi, testified about his injuries.
Cody Flint had been healthy with no underlying medical conditions before receiving Pfizer’s genetic therapy injection. His first dose was February 1, 2021. Within 30 minutes he developed a severe headache that evolved into a burning sensation in his neck. Two days later he realized something wasn’t right, but only after having taken his airplane into the air. He described what happened next:27
“I was starting to develop tunnel vision and my headache was getting worse. Approximately two hours into my flying I pulled my airplane up to turn around and felt an extreme burst of pressure in my ears. Instantly I was nearly blacked out, dizzy, disoriented, nauseous and shaking uncontrollably. By the grace of God, I was able to land my plane without incident, though I do not remember doing this.”
The doctors initially told him he had an attack of vertigo and a severe panic attack. However, without a history of either, and a continuing decline of his medical condition, the doctors then told him that ”only an adverse reaction to the Pfizer vaccination or major head trauma could have caused this much spontaneous damage.”
After one year and numerous spinal taps and two surgeries, Flint shared that the vaccine stole his career and his future. He spent all his savings to pay his medical bills and his family “is on the verge of losing everything we have.”
Statistical Tricks Behind Fear Mongering
It is important to note here that the claims made by Pfizer that the vaccine is 95% effective is not an effectiveness rating you may imagine. You might think that 95% effective means that the shot protects 95 out of 100 people.
But that is something called a relative risk reduction, which actually is the difference in event rates for both groups being studied.28 In other words, it’s the reflection of the number of vaccinated people who got COVID during the trials compared to the number who were not vaccinated. If you look at the absolute risk reduction, which is far more relevant for public health measures, you’ll see that number is actually less than 1%.29
This means that out of 100 people who got the injection, it is effective for less than one person. While this makes the vaccine of dubious benefit, it also speaks to the propaganda and fear-mongering vaccine makers and vaccines stakeholders have used to promote the dangerous shot — especially when the National Institutes of Health says absolute risk reduction “is the most useful way of presenting research results.”30
Experts Are Using Herd Immunity Reasoning to Convince Parents
Since children have little reason to get the COVID shot, health officials are spinning the idea that they should be vaccinated for the sake of herd immunity. They want you to believe that not only should you look at the people around you as vectors of disease, but also that children could be asymptomatic carriers and supposedly silently spreading a deadly disease to Grandma’s house.
What they aren’t telling you, and the media is not covering, are the studies that show children are not driving the pandemic, and in fact appear less likely to transmit COVID-19 than adults.31 The Children’s Health Defense noted:32
“In short, public health leaders say, parents must ‘vaccinate the young to protect the old.’ Given the federal government’s estimate that one vaccine injury results from every 39 vaccines administered, it seems clear that officials expect children to shoulder 100% of the risks of COVID vaccination in exchange for zero benefit.”
Herd immunity occurs when enough people have acquired immunity to an infectious disease so that it no longer is widely spread in the community. This is calculated using a reproductive number or R0.33 This is the estimated number of new infections that may occur from one infected person. R1 means that one person who is infected is expected to infect one other person.
When R0 is below 1 it indicates that cases are declining and R0 above 1 suggests that they are on the rise. While it’s far from an exact science, a person’s susceptibility to infection is known to vary depending on factors including age, health and contacts within the community.
The initial calculation for COVID-19 health intervention tracking was based on assumptions that each person had the same susceptibility and would mix randomly with others in the community. However, a study published in Nature Reviews Immunology34 suggested the herd immunity threshold for COVID-19 may need adjustment since children are less susceptible to the disease. The scientists wrote:35
“Another factor that may feed into a lower herd immunity threshold for COVID-19 is the role of children in viral transmission. Preliminary reports find that children, particularly those younger than 10 years, may be less susceptible and contagious than adults, in which case they may be partially omitted from the computation of herd immunity.”
In other words, the idea that we must vaccinate children to protect adults is not backed by evidence in this illness. After decades of studying vaccine research and holding responsible positions in health care, you would hope that individuals like Dr. Anthony Fauci,36 director of the National Institute of Allergy and Infectious Diseases and Dr. Rochelle Walensky,37 director of the Centers for Disease Control and Prevention, should understand the science.
If an assumption is made that these individuals do understand the science that doesn’t support vaccinating children, and they have at least glanced at the VAERS data collected by the CDC and FDA, then you must ask the question — what is the underlying goal of vaccinating children with a potentially lethal and disabling shot when they have an exceedingly low risk of severe COVID-19 or dying from the illness?
Sources and References
1, 31 Pediatrics, 2020;146(2)
7 Estimating the Number of COVID Vaccine Deaths in America, November 1, 2021
13 Health and Human Resources, Grant Final Report, Results page 6
17 Centers for Disease Control and Prevention, December 8, 2021, last table
19 Centers for Disease Control and Prevention, Daily Updates of Totals by Week and State
34, 35 Nature Reviews Immunology 2020, doi.org/0.1038/s41577-020-00451-5
37 Centers for Disease Control and Prevention, November 2, 2021
UK Govt Data Shows that Triple-Vaccinated Persons are More Than Four Times as Likely to Test Positive for Omicron Than Unvaccinated
/
From [HERE] According to early data published on Tuesday by the ONS, the triple-vaccinated are 4.5 times as likely to test positive for a probable Omicron infection than the unvaccinated. The double-vaccinated, meanwhile, are 2.3 times as likely to have a probable Omicron infection.
The data from the ONS Infection Survey, while provisional, adds support to the claim that the Omicron variant has significant vaccine evading ability.
Note that this is the probability of an infection being Omicron given a person is infected, so it doesn’t tell us how likely a person is to test positive in the first place. This means it doesn’t tell us that the vaccines are making things worse overall, only that they are making it much more likely that a vaccinated person is infected with Omicron than another variant. In other words, it is a measure of how well Omicron evades the vaccines compared to Delta. The fact that the triple-vaccinated are much more likely to be infected with Omicron than the double-vaccinated confirms this vaccine evading ability.
The data also doesn’t tell us anything about the severity of Omicron, or how well the vaccines continue to protect against serious disease.
It does mean, though, that the current Omicron outbreak is largely an epidemic of the vaccinated and is being driven, not by the unvaccinated, but by those who have been double and triple jabbed. Combined with the fact that Omicron has quickly grown to be the majority of new infections, it suggests the vaccinated are playing an outsize role in the current outbreak.
The complete table, with modelled data from the ONS Infection Survey, is reproduced below.
Authority Hates All Lives: A Dallas Cop Knelt on the Back of a Subdued Mentally ill White man for 14 Mins. Other Cops Watched and Joked while He was Murdered. Circuit Ct Rejects Immunity, Allows Suit
/

From [HERE] Dallas police officer continues to kneel on the back of a mentally ill man after he called 911, and long after he had been subdued and restrained. Other officers stand around, joke as the man loses consciousness and died from asphyxiation, 14 minutes later. District court: Qualified immunity. Fifth Circuit (link is external): No way. Reversed. "Within the Fifth Circuit, the law has long been clearly established that an officer’s continued use of force on a restrained and subdued subject is objectively unreasonable." The victim's mother can sue the kneeling officer and several of the others.
The case is Vicki Timpa, et al v. City of Dallas, et al(link is external), No. 20-10876 (5th Cir. Dec. 15, 2021). According to the opinion of the court:
On the evening of August 10, 2016, Timpa called 911 and asked to be picked up. He stated that he had a history of mental illness, he had not taken his medications, he was “having a lot of anxiety,” and he was afraid of a man that was with him. The call ended abruptly. When the operator called back, Timpa provided his location on Mockingbird Lane in Dallas, Texas. In the background of the call, the sounds of honking and of people arguing could be heard. A motorist then placed a 911 call to report a man “running up and down the highway on Mockingbird [Lane,] . . . stopping traffic” and attempting to climb a public bus. A private security guard called 911 with the same report and noted his belief that the man “[was] on something.” The dispatcher requested officers respond to a Crisis Intervention Training (CIT) situation and described Timpa as a white male with schizophrenia off his medications. A CIT call informs responding officers that the situation involves an individual who may be experiencing mental health issues. DPD General Orders instructed that five officers report to CIT calls to perform the “Five Man Takedown,” which is a control technique where each of four officers secures one of the subject’s limbs while a fifth officer holds the head. This technique allows officers to gain control over a subject and simultaneously prevent him from injuring himself or others. Regardless of whether officers were responding to a CIT call, DPD General Orders instructed that, for all arrestees, “as soon as [they] are brought under control, they are placed in an upright position (if possible) or on their side.” DPD General Orders reiterated this instruction for the restraint of subjects suffering from “excited delirium.” Excited delirium is “a state of agitation, excitability, and paranoia . . . often associated with drug use, most commonly cocaine.” Goode v. Baggett, 811 F. App’x 227, 233 n.6 (5th Cir. 2020) (citing Gutierrez v. City of San Antonio, 139 F.3d 441, 444 (5th Cir. 1998)). The Orders described the following symptoms as indicators of excited delirium: “[d]elusions of persecution,” “[p]aranoia,” and “[t]hrashing after restraint.” Officers were instructed to “treat the arrest of a subject [in a state of excited delirium] as a medical emergency” and to “continuously monitor[]” the arrestee because “[s]ubjects suffering from this disorder may collapse and die without warning.” The Orders commanded that subjects in a state of excited delirium “will be placed in an upright position (if possible) or on their side as soon as they are brought under control.” In addition, the Officers on the scene received specific training on excited delirium, which twice reiterated that officers must, “as soon as possible, move [the] subject to a recovery position (on [their] side or seated upright)” because the prolonged use of a prone restraint may result in “positional asphyxia.” The training also warned that “[i]f [the] subject suddenly calms, goes unconscious, or otherwise becomes unresponsive, advise [a paramedic] immediately,” because “[a] sudden cessation of struggle is a prime indicator that the subject may be experiencing fatal autonomic dysfunction (sudden death).”
Supervising Police Sergeant Kevin Mansell arrived first on Mockingbird Lane at 10:36 p.m. By that point, Timpa had already been handcuffed by two private security guards and he was sitting barefoot on the grass beside the sidewalk. Mansell called for backup and for an ambulance, stating that Timpa was “in traffic . . . and he’s definitely going to be a danger to himself.” According to Mansell, Timpa was “thrashing” on the ground, “kicking in the air [at] nobody that’s there,” and “hollering, ‘Help me, help me, God help me.’” Once, before the other Officers arrived, Timpa managed to roll into the gutter of the street and Mansell and a security guard lifted Timpa and placed him back on the grass. Within seven to ten minutes, two paramedics, Senior Corporal Raymond Dominguez, and Officers Dustin Dillard, Danny Vasquez, and Domingo Rivera arrived. Each of the Officers was informed that Timpa was a mentally ill individual off his medications. Three of the Officers (Dillard, Vasquez, and Rivera) were wearing body cameras, which captured the following fifteen minutes. The footage begins with Timpa handcuffed and barefoot on his back on the grass boulevard beside a bus bench, yelling: “Help me! . . . You’re gonna kill me!” The Officers attempted to calm Timpa. Timpa rolled back and forth on the grass, then rolled close to the curb of the street. Dillard and Vasquez immediately forced Timpa onto his stomach and each pressed one knee on Timpa’s back while a security guard restrained his legs. Vasquez removed his knee after approximately two minutes. Dillard continued to press his knee onto Timpa’s upper back in the prone restraint position for fourteen minutes and seven seconds. He pressed his left knee into Timpa’s back and his left hand between Timpa’s shoulders with his right hand pressing on Timpa’s right shoulder intermittently. In his protective vest and duty belt, Dillard weighed approximately 190 pounds.
Approximately fifteen seconds into the restraint, Dillard asked Timpa: “What did you take?” Timpa answered, “Coke.”1 One minute into the restraint, a paramedic attempted to take Timpa’s vitals. The paramedic was unable to get a reading as Timpa continued to struggle and yelled: “I can’t live!” Between three to seven minutes into the restraint, the Officers swapped out the private security guard’s handcuffs with some difficulty because of Timpa’s continued flailing.2 At the same time, the Officers zip tied Timpa’s ankles and forced his lower legs under the cover of a concrete bus bench. While the Officers were securing restraints on Timpa’s ankles, one Defendant-Officer said: “We don’t have to hogtie him, do we?” Another Defendant-Officer suggested “we could pull his legs up.” The Officers ultimately left Timpa’s legs under the bus bench. Seven minutes into the restraint, Timpa—prone and cuffed at the hands and ankles—had calmed down sufficiently for a paramedic to successfully take his vitals. When the paramedic approached, Dillard asked: “Do you want me to roll him over?” The paramedic responded: “Before y’all move him, if I can just get right here and see if I can get to his arm.”
While the paramedic was taking Timpa’s vitals, Rivera left the scene to find Timpa’s car. By the time the paramedic had finished, approximately nine minutes into the restraint, Timpa’s legs had stopped kicking, though he remained vocal and kept calling for help. Thirty seconds later, only Timpa’s head moved intermittently from side to side. He continued to cry out “Help me!” but his voice weakened and slurred. Much of what he said was too muffled to be comprehensible. Forty-five seconds later, he suddenly stilled and was quiet except for a few moans. Then, he fell limp and nonresponsive for the final three-and-a-half minutes of the restraint. The Officers discussed what to do next. Dominguez said to Mansell: “So what’s the plan? You’re [in charge] out here, sir.” Mansell responded that they should “strap [Timpa] to a gurney.” Mansell then returned to his patrol car, “a few feet [away],” to check for warrants for Timpa’s arrest. He sat in his vehicle “with the car door open.” During this time, the Officers began to express concern that Timpa was nonresponsive. Dominguez said, “Tony, are you still with us?” Vasquez said, “Is he acknowledging you anymore?” Dominguez said, “Not really.” Dillard called Timpa’s name to no response. Dominguez stated that he wanted to “mak[e] sure he was still breathing ‘cause his nose is buried in the [ground].” Dillard said, “I think he’s asleep!” and stated that he heard Timpa “snoring.” Dominguez and Vasquez expressed surprise and then made jesting comments about Timpa’s loss of consciousness. A paramedic approached and asked what happened. Dillard responded: “I don’t know. He just got quiet.” Vasquez said: “All of a sudden, just . . . bloop.” The paramedic administered a sedative and Timpa’s head twitched. Then, threeand-a-half minutes after Timpa had become nonresponsive, Dillard removed his knee. Shortly after the Officers placed Timpa on the gurney, the paramedics determined that he was dead. The Dallas County Medical Examiner conducted Timpa’s autopsy and ruled his death a homicide. The report identified cocaine in Timpa’s blood and concluded that he had been suffering from “excited delirium syndrome.” The report further concluded that Timpa died from “sudden cardiac death due to the toxic effects of cocaine and [the] physiologic stress associated with physical restraint,” which could have resulted in “mechanical or positional asphyxia.” Plaintiffs’ medical expert, Dr. Kim Collins, MD, a forensic pathologist, went one step further and concluded, “to a reasonable degree of medical certainty,” that Timpa’s death was caused by mechanical asphyxia, which occurs when an individual’s torso is compressed, preventing respiration and circulation of oxygen. She testified that Timpa’s obesity, extreme exertion, and state of excited delirium exacerbated the risk of mechanical asphyxiation. She further testified that Timpa would have lived had he been restrained for the same amount of time in a prone position without force applied to his back.
Vicki Timpa, the mother of the deceased, individually and as representative of the estate of the deceased, and Cheryll Timpa, individually and as next friend of K.T., a minor child of the deceased, filed this Section 1983 lawsuit alleging, as relevant here, a claim of excessive force against Defendant-Officer Dillard and claims of bystander liability against Defendant-Officers Mansell, Vasquez, Dominguez, and Rivera. Joe Timpa, the father of the deceased, later intervened. On summary judgment, the district court granted qualified immunity to the Officers in their individual capacity on the basis that “there was no law clearly establishing Defendants’ conduct as a constitutional violation prior to August 10, 2016.” The district court dismissed the bystander liability claims on the same basis. On appeal, the Plaintiffs argue that the district court erred in dismissing the excessive force claim and the bystander liability claims. [MORE]
$67M Jury Verdict in Landon Nobles Case Not Enough: APD Cops Shot a Black Man in the Back Several Times as a Crowd Dispersed and Left Him to Die. He Posed No Danger to Cops, Hadn't Committed a Crime
/
From [HERE] A Travis County jury last week awarded the family of Landon Nobles $67 million in damages in a wrongful death lawsuit in federal court against Austin police, who shot the 24-year-old Black man after an altercation on East Sixth Street in May 2017.
The stunning sum far surpasses any amount awarded to families of people killed by the Austin Police Department in the past decade; those payouts cumulatively total just over $8 million. Prior to the Nobles verdict, the largest sum awarded in a police excessive force case was a $3.25 million settlement in 2017 with Ketty Sully, the mother of 17-year-old David Joseph, shot and killed by an Austin police officer in February 2016.
Landon Nobles, 24 at the time, was shot and killed by Austin Police Department officers Sgt. Richard Egal and Cor. Maxwell Johnson on May 7, 2017, after a crowd dispersed from in front of bars on East Sixth Street in downtown Austin.
Witnesses in the crowd claim Nobles was not displaying a gun and posed no danger when he was shot in the back, according to the lawsuit. The lawsuit said Nobles was shot “in the back multiple times.”
According to the complaint:
On or about May 7th, 2017, Landon Nobles, a twenty-four-year-old African-American Austinite, went to 6th Street in Austin to celebrate a birthday with his cousins Royie Nobles and Frankie Nobles. At approximately 2:30 am, Landon Nobles, Royie Nobles, and Frankie Nobles noticed a crowd of people gathered near the Jackalope and Moose Knuckle Pub in the 400 block of East Sixth Street and decided to observe the crowd. There was much jockeying and posturing as two people interacted as if “fixing to fight.” A small crowd gathered around the fighters.
The crowd dispersed after a loud popping noise emanated from the crowd. Landon Nobles walked away to the nearby intersection and then after a few minutes started walking briskly away from the corner of Sixth Street and Trinity Street toward 7th and Trinity Street, when suddenly an unidentified Austin Police Officer threw a bike in front of Landon Nobles, which caused him to fall.
At no time did any officer of the Austin Police Department announce their presence or instruct Landon Nobles to stop.
As Landon Nobles attempted to regain his balance, he was subsequently shot in the back multiple times by Sergeant Richard Egal and Corporal Maxwell Johnson. According to several non-police witnesses, Landon Nobles was not displaying a gun and posed no danger to Sergeant Richard Egal, Corporal Maxwell Johnson, or anyone for that matter at the time of the shooting, or at any time at all. There is no evidence that Defendants Sergeant Richard Egal and Corporal Maxwell Johnson or any third party feared for their lives or the lives of anyone else at the time lethal force was used against Landon Nobles.
Landon was killed right there on the street and he was left to die in the gutter as he bled out from the gunshot wounds inflicted by Officers Egal and Maxwell Johnson who shot Landon in the back. Twenty minutes later, Landon Nobles was later rushed to Brackenridge Hospital by Austin-Travis EMS where he was pronounced dead at approximately 3:08 am on May 7th, 2017. 16. As a result of Sergeant Richard Egal and Corporal Maxwell Johnson’s unreasonable and senseless use of deadly force, Landon Nobles died after suffered agonizing pain.
Based on media reports, Austin Police officers use deadly force against African- American suspects at a higher rate than white suspects, even though African- Americans comprise only 8% of Austin’s population. Additionally, the Austin Police Department utilizes deadly force against unarmed individuals disproportionately when the victims are African-American.
The verdict comes as the city and its police officers face numerous excessive force lawsuits stemming from APD's violent response to peaceful Black Lives Matter protesters in the summer of 2020. The Nobles case was defended by city staff attorneys, who did not need to pay for outside counsel for the officers involved; that's not so in at least some of the BLM cases working their way through the courts.
Family Of Black Man Shot 10X by NYPD Disputes "Suicide By Cop" Claim. Bodycam n/a for 30 Days [although the Public Owns the Video, We Made Govt Our Masters and Put Them In Charge of Our Property]
/
From [HERE] The family of a Black man killed by police earlier this week is challenging the NYPD’s description of the death as a “suicide by cop situation" — calling on the department to release body camera footage of the fatal encounter.
Eudes Pierre, a 26-year-old Crown Heights resident, was shot ten times on Eastern Parkway early Tuesday morning, after allegedly charging at police officers with a pink knife. A spokesperson for the NYPD said that Pierre had called the police on himself and left behind a suicide note — a sign that he wanted officers to end his life.
During a press conference on Wednesday, Pierre’s mother, Marguerite Jolivert, spoke to reporters through tears, explaining that her son was in the throes of a mental health crisis. She accused police of rushing to pull the trigger instead of de-escalating the situation or calling crisis professionals to the scene.
“My son was sick. He had a mental disease,” said Jolivert, flanked by sobbing family members and friends. “He didn’t deserve to be killed like an animal.”A former basketball player at the College of Staten Island who was recently working for Uber Eats, Pierre was taking medication for bipolar disorder, according to his family. A police spokesperson said the department had responded to two prior calls involving Pierre, both of them believed to be suicide attempts.
His death comes as the NYPD continues to face scrutiny over its response to calls about emotionally disturbed individuals. Since 2015, at least 19 people have been killed by police while experiencing mental health emergencies, according to the advocacy group Correct Crisis Intervention Today.
In the last year, the city has experimented with a small pilot program to send emergency medical teams and social workers to non-violent mental health calls. The program showed limited success in its first six months, and Mayor-elect Eric Adams declined to embrace it while on the campaign trail.
Inquiries to both Mayor Bill de Blasio and Adams about the shooting were not returned.
Reverend Kevin McCall, a civil rights leader and spokesperson for the family, called on the department to immediately release the body camera footage.
“I guarantee you, if he was a white kid, he’d be alive today, but because he was a Black boy living under the de Blasio administration, he’s dead,” McCall said. “This is not our first rodeo of mentally ill having issues with the police.”
Just a few blocks from the site of Pierre’s death, police killed another emotionally disturbed individual, Saheed Vassell, in 2018. Both were Black men shot ten times by officers with the NYPD’s 71st precinct while enduring apparent mental health episodes.
In Pierre’s case, police said they responded to a call at 4:00 a.m. Tuesday of a man with a gun on Eastern Parkway near Utica Avenue. When officers arrived, they said Pierre refused to show his hands, instead sprinting into a nearby subway station.
When he emerged from the station, two officers attempted to deploy their stun guns to no effect. Moments later, Pierre was fatally shot by two officers.
“He ran, literally ran, at one of the officers with the knife in his hand,” NYPD Assistant Chief Michael Kemper said at a press conference earlier this week. “It was at that point where again you hear officers scream to drop the knife and the shots were fired.”
In response to requests for the body camera footage, the NYPD referred WNYC/Gothamist to a policy that gives the department 30 calendar days to make such footage public.
A spokesperson for Attorney General Tish James' Office confirmed the AG was also investigating the incident, but declined to say whether they would share the footage with the family.
At the press conference, the victim’s brother, Roland Pierre, described his young sibling as “selfless, caring, loving.”
“My brother wasn’t a criminal, he didn’t run the streets,” the elder Pierre said. “He had issues, but he was the kind of person that if you needed a dollar, he’d give it to you, even if it was his last one.”
It Goes w/o Saying that Citizens Cant Fire, Hire or Control Cops in a Police State but when the DC Police Tried To Fire 24 of Its Own Cops for Criminal Offenses Authorities Blocked Nearly Every One
/
From [HERE] The two sex workers in Washington, D.C., suspected that the drunk, bearded man in the silver Nissan Maxima was a police officer. Standing outside the car on a December night in 2015, they could see his black boots and blue cargo pants. Then there was the way he held his gun as he pointed it at them. Exactly how a cop is trained to do, one of the workers thought, according to internal police records.
After they’d called 911 reporting that a belligerent man had solicited sex, threatened one of them with a gun, and then accused them of stealing his phone, the Metropolitan Police Department officer dispatched to the scene ran the Nissan’s plates, the documents show. Sure enough, it belonged to Ronald Faunteroy, a fellow MPD officer.
The officer on the scene immediately notified Agent Charles Weeks, a 20-year veteran tasked with investigating his fellow officers. Weeks’ investigative notes suggest he threw himself into the case, seemingly dispelling any notion that there was a buddy-buddy culture within the department that would protect Faunteroy.
That very day, Weeks recorded video interviews with both of the sex workers who interacted with Faunteroy, according to Weeks’ investigative files. In the weeks that followed, he reviewed surveillance footage from two cameras in the area and interviewed every officer involved with the case. He acquired equipment records, incident reports, 911 audio, dispatch logs, and property records. He had even photocopied the notebooks of the officers responding at the scene, scouring through their chicken-scratched notes to understand what exactly happened.
He’d pieced it all together. After a grueling two-hour interview, Weeks eventually got Faunteroy to confess. Faunteroy said he’d tried to pay for sex, the records show. After being denied, he’d pointed his MPD-issued Glock at a sex worker. He’d wrongly accused her of stealing his phone. And he’d lied about it all, Weeks later determined.
“You put the puzzle together,” Faunteroy told Weeks at the end of the interview. “You’re right.”
The Metropolitan Police Department swiftly took action, moving to terminate Faunteroy. The Internal Affairs Division determined that “a preponderance of evidence existed to sustain the allegations” that he violated D.C. laws and department policy.
Yet a powerful tribunal of three high-ranking officers, known as the Adverse Action Panel, overruled the department’s decision to fire Faunteroy. The officer in charge of the panel: Robert J. Contee, who has since risen to become chief of police. Faunteroy was stripped of his title of master patrol officer, a high-ranking patrol officer paid extra to “provide effective coaching, mentoring, and guidance to other officers,” but the department roster shows he’s since regained the title.
Internal records show that MPD’s Disciplinary Review Division sought to terminate at least 24 officers currently on the force for criminal misconduct from 2009 to 2019. In all but three of those cases, the records show, the Adverse Action Panel blocked the termination and instead issued much lighter punishment – an average of a 29-day suspension without pay. These officers amassed disciplinary records for domestic violence, DUIs, indecent exposure, sexual solicitation, stalking, and more. In several instances, they fled the scenes of their crimes.
The disciplinary files, obtained by Reveal from The Center for Investigative Reporting and WAMU/DCist, provide a rare glimpse into how police officers avoid accountability and remain on the force, even after the department’s own internal affairs investigators have determined they committed crimes. The records have never before been made public.
They show:
The department’s internal investigators concluded that at least 64 people who currently serve as MPD officers committed criminal misconduct.
The department sought to terminate 24 of those officers. In 21 of the 24 cases, the Adverse Action Panel reduced their sentence to a suspension or acquittal.
The department did not seek to terminate the other 40 officers, more than half of whom the Internal Affairs Division believed had been driving either drunk or recklessly. Other criminal conduct the department did not try to fire current officers for included recklessly handling a firearm, harassment, property damage, stalking, and theft.
“These systems that MPD set up to punish or at least give officers their day in court when they committed an infraction, they don’t really work,” said Ronald Hampton, a retired MPD officer who has advocated for more accountability as a member of the city’s recently created Police Reform Commission. “It’s seated in the culture of the institution; it’s going to take more than setting up more systems within the organization to deal with it.” [MORE]
More than Half of Death-Row Prisoners Waiting to be Murdered by Authorities are Detained in Prolonged Solitary Confinement, Violating International Human Rights
/From [DPIC] More than half of all U.S. death-row prisoners are or have recently been incarcerated in prolonged conditions of solitary confinement that are likely unconstitutional and that violate international human rights norms, a DPIC analysis of data in a recent law review article has found.
In Cruel but not Unusual: The Automatic Use of Indefinite Solitary Confinement on Death Row, published in fall 2021 in the Texas Journal on Civil Liberties and Civil Rights, Merel Pontier (pictured) catalogues the conditions of confinement in each of the U.S. states that authorizes capital punishment. Pontier, who as legal director of the Clinton Young Foundation is working to free a Texas death-row prisoner whose prosecutor also secretly worked as a law clerk for the judge in his case, found that, as of late 2020 twelve U.S. states automatically housed death-sentenced prisoners in indefinite solitary confinement. She also found that, since 2017, another five states that had been sued for unconstitutional death-row conditions had ended mandatory solitary confinement.
The Death Penalty Information Center compared the populations of the death rows in those states to Bureau of Justice Statistics data on state death rows released December 10, 2021. It found that the twelve states that mandated prolonged solitary confinement — Alabama, Arkansas, Florida, Georgia, Idaho, Kansas, Mississippi, Nevada, Oklahoma, South Dakota, Texas, and Wyoming — collectively accounted for 953 death-row prisoners, or 38.6% of those on death rows nationwide at the end of 2020. An additional 338 prisoners, or 13.7% of death row, were sentenced to death in five states that, in response to prisoner lawsuits, had recently ended automatic prolonged solitary confinement. Those states are Arizona, Louisiana, Pennsylvania, South Carolina, and Virginia.
Pontier’s article reviews international human rights treaties that collectively establish minimum standards for the treatment of prisoners. These treaties, she writes, directly apply the international prohibition against “torture or other cruel, inhuman or degrading treatment or punishment” to the prison setting. In December 2015, Pontier says, the UN General Assembly adopted a set of revised standards for the treatment of prisoners, known as the Mandela Rules, that explicitly prohibit the use of prolonged or indefinite solitary confinement. The conditions death-row prisoners face in the twelve states that “automatically confine death-sentenced prisoners in isolation for twenty-two hours a day or more … [or] confine death-sentenced prisoners in isolation for just under twenty-two hours a day without meaningful human contact” without possibility of having their custody status reviewed, and the five states that recently moved away from those practices, constitute prolonged or indefinite solitary confinement, Pontier says.
Portland Protests Last Year were Filled with Undercover FBI Cops
/From [HERE] In the hours after President Biden’s inauguration this year, protesters marched once again through the streets of Portland, Ore., sending a message that putting a Democrat in the White House would not resolve their problems with a system of policing and corporate wealth that they saw as fundamentally unfair.
“No cops, no prisons, total abolition,” they chanted. Some of the activists, dressed in the trademark uniform of solid black clothing and masks that often signals a readiness to make trouble without being readily identifiable, smashed windows at the local Democratic Party headquarters.
The event — like others that had consumed the city since the murder of George Floyd by a police officer in Minneapolis in 2020 — included a variety of anarchists, antifascists, communists and racial justice activists. But there were others mingling in the crowd that day: plainclothes agents from the Federal Bureau of Investigation.
The F.B.I. set up extensive surveillance operations inside Portland’s protest movement, according to documents obtained by The New York Times and current and former federal officials, with agents standing shoulder to shoulder with activists, tailing vandalism suspects to guide the local police toward arrests and furtively videotaping inside one of the country’s most active domestic protest movements.
The breadth of F.B.I. involvement in Portland and other cities where federal teams were deployed at street protests became a point of concern for some within the bureau and the Justice Department who worried that it could undermine the First Amendment right to protest against the government, according to two officials familiar with the discussions. [MORE]
Rodney Reed Files New Petition Alleging White DA Withheld Evidence for 23 Years and Used False Testimony to Frame Him for the Murder of a White Woman, who was Actually Killed by a White Cop
/
From [DPIC] Prosecutors hid favorable evidence from Texas death-row prisoner Rodney Reed during his 1998 trial for the murder of Stacey Stites and then argued for his execution claiming that the evidence did not exist, Reed’s lawyers allege in a new court pleading filed in his case.
Reed has consistently maintained his innocence in Stites’ murder and has argued that her fiancé, Jimmy Fennell, a disgraced former police officer and a sex offender, is the killer. Reed says that he and Stites were romantically involved but hid their relationship because they feared local reaction to their interracial relationship and because Stites was engaged to a police officer with a history of racist comments.
In the latest pleading in Reed’s case, a Request for Grant of Application for Writ of Habeas Corpus filed in the 21st Judicial District Court in Bastrop County, Texas and the Texas Court of Criminal Appeals (TCCA) on December 17, 2021, Reed’s lawyers allege that Bastrop County prosecutors illegally withheld statements given by Stites’ coworkers, friends, and neighbors that would have supported Reed’s innocence claim and implicated Fennell. The filing says that for more than two decades, from before the time of trial to just before an innocence hearing in July 2021 ordered by the TCCA, prosecutors concealed witness statements from three of Stites’ coworkers, who told investigators that Reed and Stites knew each other.
Prosecutors falsely claimed at Reed’s trial that they “talked to all these people, and not one of them … ever said she was associated with that defendant. Ever. They weren’t dating according to anyone, there weren’t friends, they weren’t associates.” They argued that Stites and Reed were strangers and that he had sexually assaulted and murdered her as she was on her way to work.
The filing also reveals that Stites’ downstairs neighbor told police and a prosecutor that he frequently heard Stites and Fennell fighting. He was reportedly told “they already had their suspect, that they didn’t need nobody’s help, to mind your own business, to hush his mouth.”
Fennell — who was later convicted of sexually assaulting a woman he had detained in his police car — was initially the lead suspect in Stites’ murder. Witnesses have reported that Fennell had threatened to kill Stites if she cheated on him, and two men who met Fennell while he was imprisoned on the other charges said he confessed to murdering her.
In 1963, the U.S. Supreme Court issued a landmark ruling in Brady v. Maryland that requires prosecutors to disclose to the defense any evidence that is favorable to the defense. Withholding such evidence violates due process if there is a reasonable probability that its disclosure would have changed the outcome of the trial or sentencing, “The prosecution’s concealment of statements from Stacey Stites’s co-workers and neighbors is a textbook example of a Brady violation,” said Jane Pucher, Senior Staff Attorney at the Innocence Project, and one of Mr. Reed’s attorneys. “The constitutional violation is as crystal clear as the remedy: Rodney Reed’s conviction and death sentence must be overturned.”
The new evidence was disclosed to Reed’s defense team less than a month before his July 2021 evidentiary hearing in Bastrop County Court, 23 years after Reed was convicted and sentenced to death. Reed would have been executed without the evidence ever coming to light if the TCCA had not stayed Reed’s November 15, 2019 execution date and directed the trial court to address Reed’s claims that prosecutors secured Reed’s conviction and death sentence by suppressing exculpatory evidence and presenting false testimony.
After two weeks of testimony, Judge J.D. Langley recommended that the criminal appeals court deny Reed’s innocence claim. Judge Langley credited Fennell’s testimony at the hearing over the contrary testimony of a dozen separate defense witnesses, finding that much of their testimony was “uncredible” because the witnesses had supposedly “waited decades to bring forth [their] ‘recollection.’” The statements that were in the possession of prosecutors at the time of Reed’s trial not only bolster his version of events, but also undermine Langley’s credibility findings about the witnesses.
Langley also rejected Reed’s claim that prosecutors had presented false forensic testimony about the time of Stites’ death, crediting the trial testimony of the prosecution’s local forensic examiners over that of Reed’s nationally known forensic experts. Reed’s lawyers argue that the false testimony concerning time of death and the length of time sperm can survive in a person’s body made it appear that Reed had raped Stites just before killing her, when the evidence actually showed that Reed had consensual sex with Stites several days before she was murdered and that the killing took place at a time Fennell admitted he had been alone with her.
The TCCA has not issued a final ruling in the case.
A Black Man was Filming on His Phone. Then a Deputy Attacked Him and Charged Him With Resisting Arrest.
/From [HERE] Thousands packed the sidewalks along Veterans Memorial Boulevard in Jefferson Parish, Louisiana, watching the Krewe of Centurions Mardi Gras parade in March of 2019 when a brawl broke out at a nearby parking garage. More than two dozen men traded blows in a bloody melee that forced the parade’s 20-plus floats to grind to a halt.
Sheriff’s deputies quickly broke up the fight, arresting at least one man. As officers attempted to calm the crowd and shepherd them back to the parade route, Sgt. Keith Dowling claimed he saw someone hurling obscenities at his officers.
An “argumentative black male [was] agitating elements within the crowd by repeatedly yelling ‘Fuck You’ while gesturing with both middle fingers at responding deputies,” Dowling wrote in his incident report.
He identified the person in question as Jacobi Cage.
Cage’s presence at the parade is the only thing about that night that he and the officers agree on. Dowling, an eight-year veteran of the Jefferson Parish Sheriff’s Office, said he tried to de-escalate the situation by quietly removing Cage from the scene, but the then-20-year-old became violent and swung “wildly” at him, hitting him in the chest. The sergeant stated in his report he had no choice at that point but to use force to take Cage to the ground, after which he booked Cage for battery of an officer and resisting arrest.
After spending several hours in the parish jail, Cage was released with a summons to appear in court. He returned to his home that night feeling angry and helpless. Cage, who’d been a football standout at Destrehan High School in neighboring St. Charles Parish until his graduation two years earlier, had never been in legal trouble before, but now he was facing up to six months in jail and a criminal record.
He tried to tell his family he was innocent. He said the deputies attacked and beat him for no reason, then falsely arrested him. But it was his word against that of the Sheriff’s Office, and for a young Black man in Jefferson Parish, a majority-white, conservative community just outside of New Orleans, that was a losing hand.
As Cage lay in bed that night, unable to sleep, he scrolled through his Twitter feed and noticed a video that had been taken at the parade. The tweet said: “man just recording got assaulted and arrested for nothing.” [MORE]
Haitian Asylum Seekers Sue Biden Administration Over Encampment Conditions
/From [HERE] The Haitian Bridge Alliance (HBA) Monday filed a class action lawsuit against the Biden administration over alleged US officials’ abuse of asylum-seeking Haitians.
According to the lawsuit, the Department of Homeland Security violated thousands of Haitian asylum seekers’ rights. The suit claimed the plaintiffs fled danger and instability in Haiti, seeking asylum in the US. Upon arriving, they joined at least 15,000 Haitian asylum seekers in a makeshift US Customs and Border Protection encampment in Del Rio, Texas. Plaintiffs claimed they suffered from hunger and dehydration due to encampment conditions.
Plaintiffs alleged they “sweltered in triple-digit temperatures” by day and “slept on the ground” at night. One father, Mirard Joseph, ventured to Mexico to buy food and water for his wife and child. When he attempted to return, a “mounted officer shouted at Mirard, lashed at him with split reins, grabbed his neck, and held his collar.” About two days later, Mirard and his family were expelled to Haiti. Mirard is now hiding in Haiti, and his wife and daughter traveled to Chile seeking medical treatment for an illness allegedly developed in the encampment.
The HBA, a community-based organization, claims the US has a history of anti-Haitian immigration policies and alleges that the US “brutally deployed” Title 42 Process against Haitians. The Trump administration introducedTitle 42 Process in early 2020 as an emergency regulation under US health law. Section 265 of Title 42 provides that the Centers for Disease Control and Prevention Director may deny entry to individuals when “there is serious danger of the introduction of [a communicable] disease into the United States.” Customs officers are authorized to implement CDC immigration orders.
In October, UN human rights experts condemned the US mass expulsions policy of Haitian migrants and refugees. The experts warned that collective expulsions violate international law. A month prior, US special envoy to Haiti Daniel Foote resigned in protest over the deportation policy. Foote expressed desire “not be associated with the United States inhumane, counterproductive decision to deport thousands of Haitian refugees” to Haiti.
UN agencies also voiced concerns over premature deportations. UN Office of the High Commissioner for Human Rights (OHCHR) spokesperson Marta Hurtado expressed concern over disturbing images of Haitians being rounded up and deported. Hurtado noted on behalf of OHCHR that Haitians should be afforded individual assessments to determine their asylum status prior to deportation. She also shared fears that “some of these people have not received that protection that they needed.”
In the pending lawsuit, the HBA seeks injunctive and declaratory relief. The HBA further aims “to ensure accountability and an end to the Biden Administration’s harmful, discriminatory, and unlawful policies.”
New EJI Report Documents Racial Bias in Coverage of Crime by the Dependent Media
/
From {HERE] In collaboration with EJI, Global Strategy Group has published a report on the role of racial bias in the media as it pertains to coverage of people prosecuted in the criminal court system.
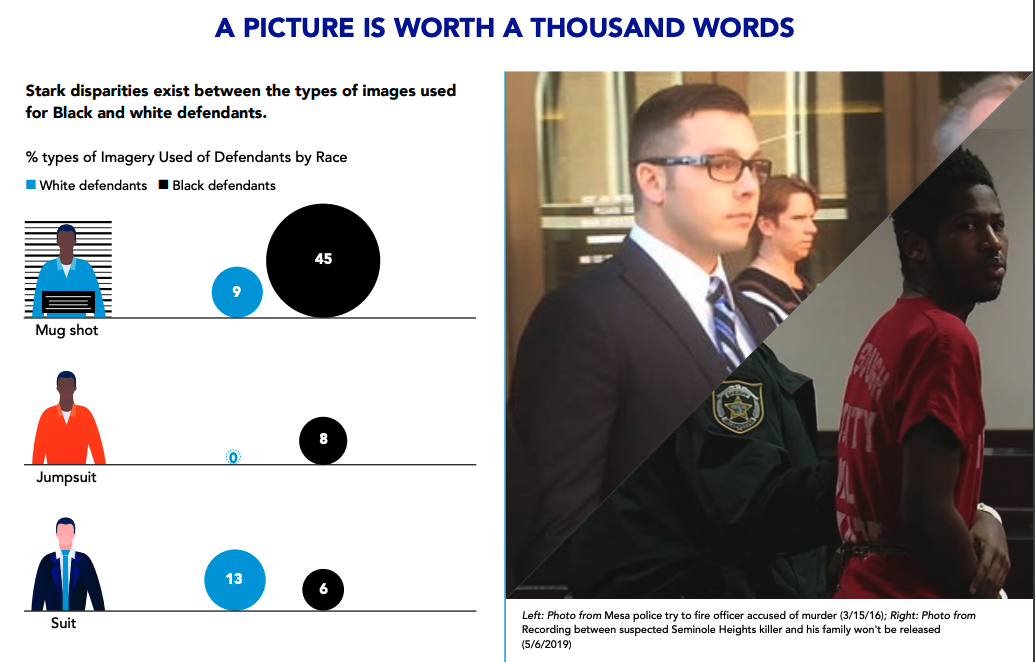
The report, Innocent Until Proven Guilty? A look at media coverage of criminal defendants in the U.S., uses data from 10 criminal cases to analyze differing portrayals of Black defendants and white defendants, resulting in unreliable court outcomes.
The data points to racial bias in over 20 different topics surrounding media coverage including the use of imagery, language choices, the framing of the accused and the victim, and reporter background.
“Racially biased media coverage has been a substantial factor contributing to unreliable and unjust outcomes in the criminal legal system,” EJI director Bryan Stevenson said. “News media have often reinforced a presumption of guilt and dangerousness assigned to Black people when reporting on crime while devaluing the lives of Black people and the harm they suffer when victimized. American media can and should do better in eliminating racially biased coverage.”
Some of the findings from the report include:
Mugshots were used in coverage of 45% of cases involving Black people accused of crimes compared to only 8% of cases involving white defendants
White victims were nearly four times more likely to be presented in photos with friends and family than Black people victimized by crime
Media coverage was 50% more likely to refer to white defendants by name as compared to Black defendants
MIT Scientist Says COVID Injections Will Kill More People than COVID. Over the Next 10-15 Years Predicts a Dramatic Spike in Lung, Heart and Brain Diseases, Blood Disorders, Strokes, Heart Failure etc
/
From [Mercola] On December 9, 2021, MIT scientist Stephanie Seneff’s paper,1 “Worse Than the Disease: Reviewing Some Possible Unintended Consequences of mRNA Vaccines Against COVID-19,” was reprinted in the Townsend Letter, the Examiner of Alternative Medicine.2 Seneff, Ph.D., a senior research scientist at MIT who has been conducting research at MIT for over five decades, has spent a large portion of her career investigating the hazards and mechanisms of action of glyphosate.
The article was originally published in the International Journal of Vaccine Theory, Practice and Research in collaboration with Dr. Greg Nigh, is still one of the best, most comprehensive descriptions of the many possible unintended consequences of the mRNA gene transfer technologies incorrectly referred to as “COVID vaccines.”
Her attention was diverted to the science of mRNA gene transfer technologies in early 2020, when Operation Warp Speed was announced. As noted in her paper, many factors that lacked precedent, yet were being implemented at breakneck speed, included:
The first-ever use of PEG in an injection
The first-ever use of mRNA gene transfer technology against an infectious agent
The first-ever “vaccine” to make no clear claims about reducing infection, transmissibility or death
The first-ever coronavirus vaccine ever tested on humans (and previous coronavirus vaccines all failed due to antibody-dependent enhancement, a condition in which the antibodies actually facilitate infection rather than defend against it)
The first-ever use of genetically modified polynucleotides in the general population
An Insanely Reckless Process
In a May 2021 interview with me, Seneff said:
“To have developed this incredibly new technology so quickly, and to skip so many steps in the process of evaluating [its safety], it's an insanely reckless thing that they've done. My instinct was that this is bad, and I needed to know [the truth].
So, I really dug into the research literature by the people who've developed these vaccines, and then more extensive research literature around those topics. And I don't see how these vaccines can possibly be doing anything good ...”
At the time, just five months into the mass inoculation campaign, Seneff suspected the COVID shots would end up killing far more people than the infection itself. Today, a full year into it, the statistics are grim beyond belief, proving her educated prediction to have been an astute one.
mRNA Jabs Are Shockingly Hazardous
As of December 3, 2021, the U.S. Vaccine Adverse Event Reporting System (VAERS) has logged an astounding 927,738 COVID jab related adverse events, including 19,886 deaths.3 VAERS can receive reports from vaccine manufacturers and other international sources, and if we exclude those, the death toll reported in U.S. territories exclusively stands at 9,136.4
Of the total death reports, Pfizer — the only company that the U.S. Food and Drug Administration has granted full licensing for an as-yet unavailable COVID shot — accounts for the vast majority: 13,268, compared to 4,894 for Moderna, 1,651 for Janssen and 73 for an undisclosed brand.
Pfizer also accounts for the vast majority of hospitalizations post-injection, and while those over the age of 66 make up the bulk of deaths, the 25-to-50 age group accounts for most of the hospitalizations. Key side effects that are now being reported in massive numbers include:5
All of these consequences were predicted by Seneff and Nigh in their paper, which makes the events all the more tragic. Importantly, VAERS is notoriously underreported, so the real-world impact of these shots is far greater than what those data suggest.
The Cure Is Indeed Worse Than the Disease
Calculations6 performed by Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, and his team of statisticians suggest VAERS COVID-related reports are underreported by a factor of 41. This is a conservative estimate, supported by calculations using a variety of sources besides VAERS itself.
That means that in the U.S. alone (using the data for U.S. territories only), the actual death toll may be closer to 374,576 (including international deaths reported to VAERS would put the death toll at 815,326), and those are deaths that occurred within days or weeks post-injection.
As Seneff and Nigh explain in their paper, there’s overwhelming reason to suspect that these gene transfer injections will have devastating impacts in the long term, resulting in excess deaths over the next decade.
What’s more, it’s clear that the death toll from the COVID-19 infection itself in the U.S. has been vastly exaggerated, as it’s based on positive PCR tests and even mere suspicion of COVID in the absence of testing. Many died from other causes and just happened to have a positive COVID test at the time of death.
Kirsch estimates the real death tally from COVID-19 to be about 50% of the reported number (which is likely conservative). This means about 380,000 Americans died from COVID-19 (rather than with COVID), whereas the COVID shots may have killed more than 374,570 in the first 11 months alone.
Seneff suspects that in the next 10 to 15 years, we’ll see a dramatic spike in prion diseases, autoimmune diseases, neurodegenerative diseases at younger ages, and blood disorders such as blood clots, hemorrhaging, stroke and heart failure.
As predicted in the title of Seneff’s paper, it seems the cure may indeed end up being worse than the disease. This is particularly true for children and young adults, who have either died or been permanently disabled by the shots by the thousands, while having an extraordinarily low risk of dying from or being seriously harmed by the infection itself.
Seneff suspects that in the next 10 to 15 years, we’ll see a dramatic spike in prion diseases, autoimmune diseases, neurodegenerative diseases at younger ages, and blood disorders such as blood clots, hemorrhaging, stroke and heart failure.
The Spike Protein Is the Most Dangerous Part of SARS-CoV-2
The reason we’re seeing all these problems from the COVID shots is because they program your cells to continuously produce SARS-CoV-2 spike protein, which we now know is the most dangerous part of the virus. Many experts noted this from the start, wondering what the vaccine developers could possibly be thinking, selecting this as the antigen for their shots.
While the mRNA injections can cause harm in many different ways, one basic problem is that they can overstimulate your immune system to the point of failure. In summary, as your cells start producing the viral spike proteins, your immune cells rally to mop up the proteins and dump them into your lymphatic system. (This is why many report swollen lymph nodes under the arms.)
The antibody response is part of your humoral immunity. You also have cellular immunity, which is part of your innate immune system. Your innate immune system is very powerful. If you're healthy, it can clear viruses without ever producing a single antibody. Antibodies are actually a second-tier effect when your innate immune system fails.
The problem is that your innate immune system will not be activated and likely will fail to protect you if you get a COVID-19 shot, because it’s bypassing all of the areas where your innate immune system would be brought to bear.
Normally you breathe the virus in and stimulate the production secretory IgA antibodies that protect your respiratory system. When you bypass that route of exposure with a jab in the arm, no secretory IgA antibodies are produced, leaving you susceptible to the infection.
As explained by Ronald Kostoff in an excellent December 8, 2021, Trial Site News article, “COVID-19 ‘Vaccines’: The Wrong Bomb Over the Wrong Target at the Wrong Time”:7
“An effective vaccine would focus on cellular immunity in the respiratory and intestinal tract, in which secretory IgA is produced by your lymphocytes that are located directly underneath the mucous membranes that line the respiratory and intestinal tract.
The antibodies produced by these lymphocytes are ejected through and to the surface of the linings. These antibodies are thus on site to meet air-borne viruses and they may be able to prevent viral binding and infection of the cells.
Unfortunately, the main inoculants used presently for COVID-19 focus on antibodies (IgG and circulating IgA) that occur in the bloodstream. These antibodies protect the internal organs of the body from infectious agents that try to spread via the bloodstream.”
When you are injected with the COVID jab, your body will only induce IgG and circulating IgA — not secretory IgA, and these types of antibodies do not effectively protect your mucous membranes from SARS-CoV-2 infection. So, as noted by Kostoff, the breakthrough infections we’re now seeing “confirm the fundamental design flaws” of this gene transfer technology.
“A natural infection with SARS-CoV-2 (coronavirus) will in most individuals remain localized to the respiratory tract,” Kostoff writes.8 “The vaccines used presently cause cells deep inside our body to express the viral spike protein, which they were never meant to do by nature.
Any cell which expresses this foreign antigen on its surface will come under attack by the immune system, which will involve both IgG antibodies and cytotoxic T-lymphocytes. This may occur in any organ, but the damage will be most severe in vital organs.
We are seeing now that the heart is affected in many young people, leading to myocarditis or even sudden cardiac arrest and death. In other words, we are dropping the wrong bomb on the wrong target at the wrong time!”
In the end, your body will essentially believe that your innate immune system has failed, which means it must bring in the backup cavalry. In essence, your body is now overreacting to something that isn’t true. You’re not actually infected with a virus and your innate immune system has not failed, but your body is forced to respond as if both are true.
Effects Likely to Persist Long Term
What’s more, the synthetic RNA in the mRNA vaccines contains a nucleotide called methyl-pseudouridine, which your body cannot break down, and the RNA is programmed to trigger maximum protein production. So, we’re looking at completely untested manipulation of RNA.
It is very important to recognize that this is a genetically engineered mRNA for the spike protein. It is not identical to the spike protein mRNA that SARS-Cov-2 produces. It’s been significantly altered to avoid being metabolized by your body.
The spike protein your body produces in response to the COVID-19 vaccine mRNA locks into your ACE2 receptor. This is because the genetically engineered new spike protein has additional prolines inserted that prevent the receptors from properly closing, which then cause you to downregulate ACE2. That’s partially how you end up with problems such as pulmonary hypertension, ventricular heart failure and stroke.9,10
As noted in a 2020 paper,11 there’s a “pivotal link” between ACE2 deficiency and SARS-CoV-2 infection. People with ACE2 deficiency tend to be more prone to severe COVID-19. The spike protein suppresses ACE2,12 making the deficiency even worse. According to Seneff, the gene transfer injections essentially do the same thing, and we still don’t know how long the effects last.
Manufacturers initially guessed the synthetic RNA might survive in the human body for about six months. A more recent investigation found the spike protein persisted in recovered COVID patients for 15 months.13
This raises the suspicion that the synthetic and more persistent mRNA in the COVID shots may trigger spike protein production for at least as long, and probably longer.14 What’s more, the number of spike proteins produced by the shots is far greater than what you experience in natural infection.
As explained by Dr. Peter McCullough,15 this means that after your first shot, your body will produce spike protein for at least 15 months. But, when you get shot No. 2 a few weeks later, that shot will cause spike protein production to go on for 15 months or longer. With shot No. 3 six months after that, you produce spike protein for yet another 15 months.
With regular boosters, you may never rid your body of the spike protein. All the while, it’s wreaking havoc with your biology. McCullough likens it to “a permanent install of an inflammatory protein in the human body,” and inflammation is at the heart of most if not all chronic diseases. There’s simply no possible way for these gene transfer shots to improve public health. They’re going to decimate it.
Long-Term Neurological Damage Is To Be Expected
In her paper,16 Seneff describes several key characteristics of the SARS-CoV-2 spike protein that suggests it acts as a prion. This could help explain why we’re seeing so many neurological side effects from the shots. According to Seneff, the spike protein produced by the COVID shot, due to the modifications made, may actually make it more of a prion than the spike protein in the actual virus, and a more effective one.
For a detailed technical description of this you can read through Seneff’s paper, but the take-home message is that COVID-19 shots are instruction sets for your body to make a toxic protein that will eventually wind up concentrated in your spleen, from where prion-like protein instructions will be sent out, radically increasing your risk of developing neurodegenerative diseases.
Lung, Heart and Brain Diseases Are Predictable Consequences
Seneff also goes into great detail describing how the spike protein acts as a metabolic poison. While I recommend reading Seneff’s paper in its entirety, I’ve extracted some key sections below, starting with how the spike protein can trigger pathological damage leading to lung damage and heart and brain diseases:17
“The picture is now emerging that SARS-CoV-2 has serious effects on the vasculature in multiple organs, including the brain vasculature … In a series of papers, Yuichiro Suzuki in collaboration with other authors presented a strong argument that the spike protein by itself can cause a signaling response in the vasculature with potentially widespread consequences.
These authors observed that, in severe cases of COVID-19, SARS-CoV-2 causes significant morphological changes to the pulmonary vasculature … Furthermore, they showed that exposure of cultured human pulmonary artery smooth muscle cells to the SARS-CoV-2 spike protein S1 subunit was sufficient to promote cell signaling without the rest of the virus components.
Follow-on papers showed that the spike protein S1 subunit suppresses ACE2, causing a condition resembling pulmonary arterial hypertension (PAH), a severe lung disease with very high mortality … The ‘in vivo studies’ they referred to … had shown that SARS coronavirus-induced lung injury was primarily due to inhibition of ACE2 by the SARS-CoV spike protein, causing a large increase in angiotensin-II.
Suzuki et al. (2021) went on to demonstrate experimentally that the S1 component of the SARS-CoV-2 virus, at a low concentration … activated the MEK/ERK/MAPK signaling pathway to promote cell growth. They speculated that these effects would not be restricted to the lung vasculature.
The signaling cascade triggered in the heart vasculature would cause coronary artery disease, and activation in the brain could lead to stroke. Systemic hypertension would also be predicted. They hypothesized that this ability of the spike protein to promote pulmonary arterial hypertension could predispose patients who recover from SARS-CoV-2 to later develop right ventricular heart failure.
Furthermore, they suggested that a similar effect could happen in response to the mRNA vaccines, and they warned of potential long-term consequences to both children and adults who received COVID-19 vaccines based on the spike protein.
An interesting study by Lei et. al. (2021) found that pseudovirus — spheres decorated with the SARS-CoV-2 S1 protein but lacking any viral DNA in their core — caused inflammation and damage in both the arteries and lungs of mice exposed intratracheally.
They then exposed healthy human endothelial cells to the same pseudovirus particles. Binding of these particles to endothelial ACE2 receptors led to mitochondrial damage and fragmentation in those endothelial cells, leading to the characteristic pathological changes in the associated tissue.
This study makes it clear that spike protein alone, unassociated with the rest of the viral genome, is sufficient to cause the endothelial damage associated with COVID-19. The implications for vaccines intended to cause cells to manufacture the spike protein are clear and are an obvious cause for concern.”
The COVID Shots Activate Latent Viruses
As mentioned earlier, shingles infection is turning out to be a rather common side effect of the COVID shot, and like the neurological, vascular and cardiac damage we’re seeing, activation of latent viral infections was also predicted.
One reason why latent viral infections are cropping up in response to the shots is because the shots disable your type I interferon pathway. A second reason is because your immune system is overburdened trying to deal with the inflammatory spike proteins flowing through your body. Something’s got to give, so latent viruses are allowed to break through.
That’s not the end of your potential troubles, however, as these coinfections may worsen or accelerate other conditions, such as Bell’s Palsy, myalgic encephalomyelitis and chronic fatigue syndrome.
Herpes viruses, for example, have been implicated as a trigger of both AIDS18 and chronic fatigue syndrome.19 Some research suggests these diseases don’t appear until viruses from different families partner up and the type 1 interferon pathway is disabled.
With all of that in mind, it seems inevitable that, long term, the COVID mass injection campaign will result in an avalanche of a wide range of debilitating chronic illnesses.
Sources and References
1 International Journal of Vaccine Theory, Practice and Research May 10, 2021; 2(1): 38-79
4 OpenVAERS data as of December 3, 2021. For US only data, flip the selection switch at top
11 European Journal of Internal Medicine June 2020; 76:14-20
14, 15 New American November 8, 2021 , video at circa 8 minutes
16, 17 International Journal of Vaccine Theory, Practice and Research May 10, 2021; 2(1): 402-444
18 Journal of Antimicrobial Chemotherapy 1996 37. Suppl B, 87-95
CDC Data Shows that COVID Injections Have Caused at Least 965,843 "Adverse Events," including 20,244 Deaths and 33,675 People have been Permanently Disabled (only 1% of adverse events are reported)
/From [CHD] The Centers for Disease Control and Prevention today released new data showing a total of 965,843 reports of adverse events following COVID vaccines were submitted between Dec. 14, 2020, and Dec. 10, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 20,244 reports of deaths — an increase of 358 over the previous week — and 155,506 reports of serious injuries, including deaths, during the same time period — up 4,560 compared with the previous week.
Excluding “foreign reports” to VAERS, 691,884 adverse events, including 9,295 deaths and 59,767 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Dec. 10, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 9,295 U.S. deaths reported as of Dec. 10, 21% occurred within 24 hours of vaccination, 26% occurred within 48 hours of vaccination and 61% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 480 million COVID vaccine doses had been administered as of Dec. 10. This includes279 million doses of Pfizer, 184 million doses of Moderna and 17 million doses of Johnson & Johnson (J&J).
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events. [MORE]