'Feel Free to Say Nothing Bad About the Vaccines.' Sen Elizabeth Warren Sued for Pressuring Amazon to Stop Selling Book, ‘The Truth About COVID-19.’ Violent Do-Gooder Seeks to Control Speech/Thought
/
From [HERE] In early September 2021, U.S. Sen. Elizabeth Warren sent a letter to Andy Jassy, chief executive officer of Amazon.com, demanding an “immediate review” of Amazon’s algorithms to weed out books peddling “COVID misinformation,” stressing that Amazon’s sale of such books was “potentially unlawful.”
Warren specifically singled out the book, “The Truth About COVID-19,” co-written with Ronnie Cummins, founder and director of the Organic Consumers Association (OCA), as a prime example of “highly-ranked and favorably-tagged books based on falsehoods about COVID-19 vaccines and cures” that she wants banned.
As a government official, it is illegal for Warren to violate the U.S. Constitution, and pressuring private businesses to do it for her is not a legal workaround.
Cummins and I, along with our publisher, Chelsea Green Publishing, and Robert F. Kennedy Jr., who wrote our foreword, are now suing Warren, both in her official and personal capacities, for violating our First Amendment rights and scaring book sellers into pulling and/or suppressing sales of our book.
Ironically, Warren’s claims of misinformation are themselves misinformation that puts lives at risk.
In early September 2021, U.S. Sen. Elizabeth Warren sent a letter to Andy Jassy, chief executive officer of Amazon.com, demanding an “immediate review” of Amazon’s algorithms to weed out books peddling “COVID misinformation,” stressing that Amazon’s sale of such books was “potentially unlawful.”
Warren specifically singled out my book, “The Truth About COVID-19,” co-written with Ronnie Cummins, founder and director of the Organic Consumers Association (OCA), as a prime example of “highly-ranked and favorably-tagged books based on falsehoods about COVID-19 vaccines and cures” that she wanted banned.
“Dr. Mercola has been described as ‘the most influential spreader of coronavirus misinformation online,” Warren wrote, adding:
“Not only was this book the top result when searching either ‘COVID-19’ or ‘vaccine’ in the categories of ‘All Departments’ and ‘Books’; it was tagged as a ‘Best Seller’ by Amazon and the ‘#1 Best Seller’ in the ‘Political Freedom’ category.
“The book perpetuates dangerous conspiracies about COVID-19 and false and misleading information about vaccines. It asserts that vitamin C, vitamin D and quercetin … can prevent COVID-19 infection … And the book contends that vaccines cannot be trusted …”
Warren fancies herself above the law
Warren should know that as a government official, it is illegal for her to violate the U.S. Constitution, and pressuring private businesses to do it for her is not a legal workaround.
Since she willfully ignores the law, Cummins and I, along with our publisher, Chelsea Green Publishing, and Robert F. Kennedy Jr., who wrote our foreword, are suing Warren, both in her official and personal capacities, for violating our First Amendment rights.
The federal lawsuit, in which Warren is listed as the sole defendant, was filed in the state of Washington. As noted in our complaint:
“Once upon a time, the First Amendment was understood to guarantee that books challenging governmental orthodoxy could be sold without fear of governmental intimidation or reprisal.
“Almost sixty years ago, in Bantam Books v. Sullivan, 372 U.S. 58 (1963), the Supreme Court held that state officials violated the First Amendment by sending letters to booksellers warning that the sale of certain named books was potentially unlawful.
“The ‘vice’ in such letters and in the ‘veiled threat’ of legal repercussions they communicated, explained the Court, is that they allow government to achieve censorship while doing an end-run around the judiciary, ‘provid[ing] no safeguards whatever against the suppression of … constitutionally protected’ speech, thus effecting an unconstitutional ‘prior restraint.’
“It made no difference that the officials who sent the letter lacked the ‘power to apply formal legal sanctions’ — i.e., that the officials did not themselves have the power to sanction or prosecute the booksellers in any way. Indeed this fact made the unconstitutionality more apparent.
“The officials ‘are not law enforcement officers; they do not pretend that they are qualified to give or that they attempt to give distributors only fair legal advice … [T]hey acted … not to advise but to suppress.’
“It also made no difference, the Court expressly found, that the letters were framed as mere ‘exhort[ation]’ or that the booksellers were in theory ‘free’ to ignore the letters, because the officials had ‘deliberately set about to achieve the suppression of publications deemed ‘objectionable’,’ and ‘people do not lightly disregard public officers’ veiled threats.’
“Today, certain members of the United States Congress have apparently forgotten, or think they are above, the law set forth in Bantam Books.”
Warren’s Attack on Constitutionally Protected Speech
There’s no doubt our book, “The Truth About COVID-19,” is constitutionally protected speech, and that Warren’s letter is calling on Amazon to suppress protected speech.
In our book, we share viewpoints, ideas, opinions, verifiable facts and factual hypotheses that our federal government just so happens to disfavor, as it counters their chosen narrative that SARS-CoV-2 emerged naturally, cannot be prevented by any means other than experimental gene therapy, and cannot be treated by any other means than certain experimental and exorbitantly costly drugs.
Since the start of the pandemic, government has systematically sought to suppress the kind of information shared in our book, using the same tactic as Warren used against us here — warning internet-based companies that if they don’t censor these views, the full weight of the government’s wrath will be turned against them. As explained in our complaint:
“The term ‘vaccine misinformation’ as Warren uses it is propagandistic and false. As she uses it, ‘vaccine misinformation’ refers to any speech challenging the safety and efficacy of the COVID vaccines, even when that speech consists of factually accurate information or protected opinion …
“On September 10, 2021, as a direct result of Warren’s letter, a major national bookseller chain, Barnes and Noble, notified the publisher of The Truth About COVID-19 by email that it would no longer sell the work as an e-book. Barnes and Noble has — for now — reversed that decision.
“It is impossible for Plaintiffs to know with certainty whether, as a result of Warren’s letter, Amazon is now covertly demoting, downgrading, or otherwise suppressing The Truth About COVID-19 in numerous ways that would be hidden from view, but Plaintiffs believe that Amazon is in fact covertly taking such action.
“Even if no bookseller in the country had yielded to Warren’s threats, her letter would still be actionable as a clear violation of the First Amendment.
“In Backpage.com, LLC v. Dart, 807 F.3d 229 (7th Cir. 2015) (Posner, J.), relying on Bantam Books, the Court held that a governmental official ‘violates a plaintiff’s First Amendment rights’ if by ‘threat’ or ‘intimidation’ the official attempts to induce ‘a third party’ to stop ‘publishing or otherwise disseminating the plaintiff’s message,’ and emphasized that ‘such a threat is actionable and thus can be enjoined even if it turns out to be empty — the victim ignores it, and the threatener folds his tent.’
“Such threats go ‘by the name of ‘prior restraint,’ and a prior restraint is the quintessential first-amendment violation.’ Accordingly, Plaintiffs ask this Court to vindicate clearly established law, to vindicate Plaintiffs’ constitutional rights, to vindicate the First Amendment itself, by declaring Warren’s conduct unconstitutional and by enjoining her from repeating such conduct in future.”
Warren calls out ‘misinformation’ with misinformation
In our complaint, we also emphasize the fact that Warren’s claims of misinformation are themselves misinformation. For example, Warren claims our book falsely “asserts that … vitamin D … can prevent COVID-19 infection.” According to Warren, this claim has no scientific basis. This is clearly and verifiably false as there are many studies, published in 2020 and 2021, supporting this claim.
For example, in May 2021, the National Institutes of Health’s website, PubMed.gov, published a Journal of Medical Virology article titled “Vitamin D Deficiency Is Associated With COVID-19 Positivity and Severity of the Disease.” Many other scientific articles have also linked vitamin D deficiency with a higher risk of COVID infection, more severe outcomes and increased rates of death.
Indeed, a recent systematic review of the literature, posted on the U.S. National Library of Medicine, which is another National Institutes of Health website, concluded that “blood vitamin D status can determine the risk of being infected with COVID-19, seriousness of COVID-19, and mortality from COVID-19.
Therefore, maintaining appropriate levels of Vitamin D through supplementation or natural methods … is recommended for the public to be able to cope with the pandemic.” As noted in our complaint:
“Thus while Warren professes to champion true COVID information to save lives, she is purveying false information that could lead to COVID deaths. Warren is telling people that vitamin D levels don’t matter for COVID, when in fact — as readers would learn from The Truth About COVID-19 — correcting vitamin D deficiencies could save their lives.
“By her own logic and according to her own demands, every major social media platform should have banned Warren’s letter as ‘COVID misinformation.’ But officials like Warren only denounce ‘COVID misinformation,’ demand its censorship, and threaten legal repercussions when the statements in question challenge the COVID narrative they support — not when they themselves are misrepresenting the truth about COVID-19.
“Warren’s letter further accuses The Truth About COVID-19 of disseminating ‘false and misleading information about vaccines,’ including by (in Warren’s words) ‘contend[ing] that vaccines cannot be trusted.’
“The book’s stated thesis about the COVID vaccines is that their effectiveness ‘has been wildly exaggerated and major safety questions have gone unanswered.’ This statement is accurate and well within the bounds of constitutionally protected opinion …
“Warren’s letter further cites a June, 2021, review of The Truth About COVID-19 that purports to list examples of the book’s ‘misinformation,’ the first of which is the following: ‘the authors argue that the SARS-CoV-2 coronavirus was engineered in a laboratory in Wuhan, China.’ It is true that The Truth About COVID-19 argues that that ‘the preponderance of evidence’ supports the lab-leak theory of the origins of the COVID virus.
“But the claim that this position is ‘misinformation’ is, once again, itself misinformation. The lab-leak theory — long denounced as a ‘conspiracy theory’ by federal actors and suppressed on social media — is in fact supported by substantial and growing evidence.
“See, e.g., Wall St. Journal, ‘Science Closes In on Covid’s Origins: Four studies — including two from WHO — provide powerful evidence favoring the lab-leak theory,’ Oct. 5, 2021.
“The review’s next example of the supposed ‘misinformation’ in the The Truth About COVID-19 is this: the book ‘insists multiple times that the public health measures and restrictions will be permanent. Not true. The CDC announced that fully vaccinated Americans could resume activities without wearing masks or physically distancing, resume domestic travel, and refrain from quarantine even when following a known exposure to the virus if they remain symptom-free.’
“This CDC announcement obviously proved to be false, while the prediction made in The Truth About COVID-19 that health restrictions would continue after vaccination has proved more accurate.
“Moreover, it is not the case that the Truth About COVID-19 ‘insists’ that these restrictions will be permanent — it says that certain restrictions on our liberty, beginning in the pandemic, will ‘probably’ be permanent, reflecting a humility about the certainty of one’s assertions that Warren might have profited from.” [MORE]
More People are Dying in 2021 Everywhere Vaccines were Introduced. Johns Hopkins Data from 30 Countries Shows Vaccines are Causing Death. Statistician who Made Findings Now Banned from Twitter
/
From [HERE] and [HERE] The mass vaccination campaign against coronavirus, which started in late 2020-early 2021, has excellent, statistical support. With rare exceptions, all countries of the world (even economically backward ones) have established systems for statistical accounting of vaccinations against COVID-19.
The latest data is promptly given on the number of doses of drugs injected into people; the number of partially and completely (usually two doses) vaccinated; the proportion of vaccinated in relation to the total population of the country. Sometimes a breakdown is also given by age groups and types of injected vaccines.
The data of national vaccination statistics are collected and consolidated by some organisations that quickly give a general picture of the world and regions. Johns Hopkins University (USA) is considered one of the most authoritative centres for the accumulation and processing of statistical information on the COVID-19 pandemic and vaccination against this virus.
A huge amount of statistical information on the topic of the pandemic and vaccination is accumulating, but, alas, there are very few serious analyses of these data sets.
Therefore, the posting earlier this month on the Internet of a video entitled "COVID Deaths Before and After Vaccination Programs" did not go unnoticed. This is not a documentary or filming of some events in the world. This is a video representation of a series of graphs compiled on the basis of statistical data from Johns Hopkins University.
The author of calculations and graphs is Joel Smalley, an English analyst and a specialist in quantitative data processing. The Englishman processed statistics on forty countries and revealed the same pattern: these countries experience sharp spikes in new diseases and deaths from COVID-19 after a large batch of COVID-19 vaccines is introduced into them.
Shortly after releasing his analysis and subsequent related postings Twitter suspended him and he seems to have been disappeared from social media altogether.
Question– Why is mortality in Scotland higher in 2021 than 2020?
Answer– Because more people are dying. And the reason more people are dying is because more people have been vaccinated. In other words, there’s a link between rising mortality and the Covid-19 vaccine.
Question– You can’t prove that.
Answer– You’re right, I can’t. The evidence is all circumstantial. But it is compelling, all the same. For example, rising mortality isn’t just happening in Scotland. It’s happening in many of the countries that launched mass vaccination campaigns earlier in the year. They’re all seeing a significant uptick in all-cause mortality. Why is that? What are they doing differently in 2021 than they did in the years before?
Question– I can see what you’re getting at, but I still don’t think you have enough evidence to make your case.
Answer– Okay, then you tell me: Why are more people dying in 2021 than 2020? And, keep in mind, all-cause mortality isn’t just up a bit; it’s smashing the five-year average. Check out this recent post from Alex Berenson at Substack:
Scotland is 87% adult vaccinated; weekly deaths are now 30% above normal
Oct 14, This is from the Public Health Scotland’s Covid-19 Daily Dashboard:
“The 315 excess deaths logged last week represents a 30% increase on the five-year pre-pandemic average for this time of year. This marks the 20th consecutive week with excess deaths above the five-year average and the highest since the week ending January 10, 2021.”
Even excluding Covid deaths they were almost 20% above normal for the most recent week, and the trend is rising.” (“Scotland is 87% adult vaccinated; weekly deaths are now 30% above normal”, Alex Berenson Substack)
Question– But how can you build a case on data from just one country? It’s ridiculous.
Answer– But it’s not just Scotland. The same rule applies to many of the countries that launched vaccination campaigns earlier in the year. Here’s more from Berenson:
Add Germany – Europe’s most populous nation – to the countries seeing unusually high all-cause mortality that is NOT Covid-related.
In September, Germany reported almost 78,000 deaths, more than 10 percent higher than the expected figure, German government demographers said earlier this week.
Press: “Mortality figures (in Germany) in September, 2021: 10% above the median of previous years.” (“It’s not just the UK; all-cause deaths are also now running well above normal in Germany (80% adults fully vaccinated)”, Alex Berenson Substack)
And then there’s this is from Data Analyst’s Twitter account (check out the charts):
Data Analysis @Data_is_Louder
·
Oct 26
COVID mystery Denmark, Finland and Norway excess deaths are higher than in their worst Covid outbreak. These mysterious excess deaths happened in time conjunction with vaccination rollout.
Denmark ––“5 months is a row 2021 has broken the 10-year record of people dying from all causes…..Covid-19 deaths close to zero during the same period.”
The same is true in Ireland, UK and Israel. Take a look at England (Ages 10 to 59 years old.)
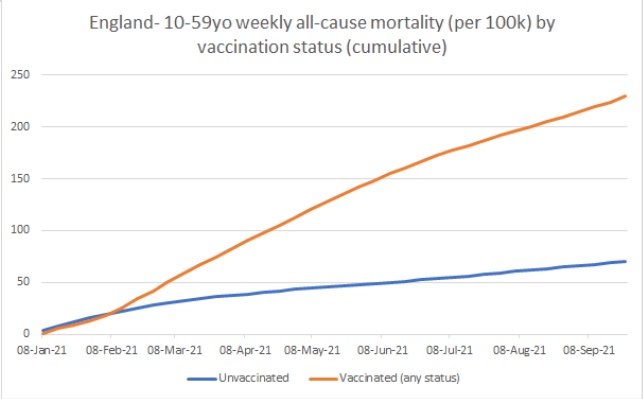
What’s so disturbing about this chart is that it shows how the vaccines target the young. “While the COVID death toll has been largely confined to the elderly… it’s the young who are bearing the brunt of vaccine injury. According to VigiAccess, the adverse event database for the World Health Organization, 41% of the more than 2.4 million vaccine injuries reported so far are among those under age 44, and just six percent are among people over age 75.” (“The real pandemic has just begun, and it’s COVID shot-induced heart attacks in the young”, Lifesite News)
That’s something you’re not going to read in the media, and for good reason, too. Because it would undermine their lethal objective to continue hyping the vaccine.
Here’s more from quantitative analyst Joel Smalley:
Weekly deaths update from the CDC. “Despite” being over 80% fully vaccinated, since 24-July, over 65s deaths in Florida are 14% higher than same period last year. “Despite” at least 50% full vaccination in the under 65s, deaths are up 46% and will rise as reporting catches up.
The examples are everywhere across the Internet. You don’t have to look very far. Wherever mass vaccinations took place, there, too, morality has risen. And–once again–these are not Covid deaths. These are mainly heart attacks, strokes, blood clots, circulatory diseases and neurological issues; the same vaccine-induced ailments we were warned about by the physicians and scientists who’ve been telling us the truth from the start. Turns out they were right after all.
Simply put, the vaccines are increasing fatalities, not reducing them. They are making matters worse not better. They are perpetuating the crisis not ending it.
And that is why the red line in the chart is pointing upward. It’s an indication that the death toll will continue to rise as long as we continue to do what we are doing now, inoculating millions of people with a cytotoxic pathogen that triggers blood clots, inflammation and autoimmunity. Here’s another chart of Scotland with a short comment from The Daily Skeptic:

“…. the presence of a Covid epidemic was not seen in summer 2020, but is seen in summer 2021. What differs between the two years? The glaringly obvious answer is the rollout of COVID-19 vaccination. There was no COVID-19 vaccination programme in 2020, but there was rollout of Covid vaccinations in a sequential way to increasingly younger age groups in 2021, a pattern that we see in the manifestation of excess deaths. …. The Yellow Card adverse events reporting system,…. has already recorded over 1,700 deaths in the U.K. population associated with the COVID-19 vaccines. There is therefore a prima facie case for COVID-19 vaccination being a contributing factor to the dramatic rise in summer excess deaths in Scotland in 2021.”
(“Are Vaccines Driving Excess Deaths in Scotland, a Professor of Biology Asks”, The Daily Skeptic)
Have you noticed how the media is trying to cover-up the sudden surge in mortality?
Here’s a good example from an article at the UK Telegraph:
“While focus remains firmly fixed on Covid-19, a second health crisis is quietly emerging in Britain. Since the beginning of July, there have been thousands of excess deaths that were not caused by coronavirus. According to health experts, this is highly unusual for the summer.Although excess deaths are expected during the winter months, when cold weather and seasonal infections combine to place pressure on the NHS, summer generally sees a lull.
This year is a worrying outlier.
According to the Office for National Statistics (ONS), since July 2 there have been 9,619 excess deaths in England and Wales, of which 48 per cent (4,635) were not caused by Covid-19.
So if all these extra people are not dying from coronavirus, what is killing them?
Data from Public Health England (PHE) shows that during that period there were 2,103 extra death registrations with ischemic heart disease, 1,552 with heart failure, as well as an extra 760 deaths with cerebrovascular diseases such as stroke and aneurysm and 3,915 with other circulatory diseases.” (“Thousands more people than usual are dying … but it’s not from Covid“, Telegraph)
So, according to the article, there were:
24% more heart failure deaths than baseline
19% ischaemic heart disease
16% cerebrovascular disease (strokes)
18% other circulatory diseases [MORE]
UK Government Data Shows Only 6 Children w/No Underlying Health Conditions Died from COVID During a 12 Month Period. Contrary to Relentless Propaganda Children Have a 99.9% Chance of Surviving Virus
/
From [HERE] and [HERE] Only six healthy children with no underlying health conditions died as a direct result of catching Covid during a 12-month window, NHS analysis has revealed.
Four died from Covid, while two developed a Kawasaki-like inflammatory condition called Pims-TS, caused by the virus.
The data calls into question the wisdom of closing schoolsand forcing children to spend months at home when the health risk to under-18s is so small.
Experts from NHS England, Public Health England and several universities and hospitals analysed official death figures in England between March last year and this February.
Their findings, published in the journal Nature Medicine on Thursday, showed that more than 3,100 children died during the study period, but only 61 had Covid.
Further examination of death certificates and medical records by independent clinical experts revealed that 25 of the 61 died due to the virus, with the six healthy children a sub-cohort of the 25. The infection played no role in 60 per cent of the recorded Covid deaths.
Prof Russell Viner, one of the study authors and professor of adolescent health at University College London, said: “Any death of a child is one too many, but we sadly must recognise that there are over 3,000 deaths of children and young people in England in ordinary years.
“The great majority of those who died were children and young people we know are sadly at much higher risk of death due to other serious medical conditions. I emphasise that this doesn’t mean children with allergies or asthma, but those very small groups who were vulnerable to winter viruses in any previous year.”
Children ‘have 99.995 per cent chance’ of surviving virus
Fifteen of the Covid/Pims-TS deaths – 60 per cent – were in children considered to be in a “life-limiting” condition, and 19 had a chronic condition. The virus “did not contribute to death” for the majority of the cases where it is listed on a child’s death certificate, the researchers said.
They also said that, during the study period, almost half a million under-18s contracted Covid, giving an infection fatality rate of five per 100,000 people. That means that if a child tests positive for the virus, they have a 99.995 per cent chance of surviving.
With more than 12 million under-18s in England, the researchers said Covid kills two children per million, meaning there is a 0.0002 per cent of a child dying from the virus.
The majority of the children – 72 per cent – who did die due to Covid were older than 10, and only two infants younger than 12 months died from the infection. In contrast, in non-Covid deaths, 46 per cent of all child deaths were in babies less than four weeks old.
Just 16 of the 25 children who died from Covid had comorbidities in two or more body systems and neurological conditions were the most common, affecting 13 people.
“All 13 [children] who died of Sars-Cov-2 with a neurological comorbidity had a complex neurodisability due to a combination of an underlying genetic or metabolic condition, hypoxic ischemic events or prematurity,” the researchers wrote.
“Eight of the 13 who had a neurological comorbidity also had a respiratory comorbidity, including five who required home respiratory support, four with non-invasive ventilation or high-flow oxygen and one with low-flow oxygen.”
No Covid deaths in under-18s with Type 1 diabetes
The study revealed that there were no Covid deaths in under-18s with Type 1 diabetes or Down’s syndrome. None of the 25 children who died from the virus suffered with an isolated respiratory condition such as asthma.
There were children who died who had asthma, but these all had other health conditions and the experts deemed that asthma did not contribute to their death.
While the research was comprehensive and spanned England, it looked only at a time period where the alpha and original strains of the virus were present as the delta variant had yet to take off in the UK.
Delta is more infectious than its predecessors, and child and adolescent infection rates in children have rocketed this year compared to last. However, as yet there is no comparable analysis for the true number of Covid deaths post-February 2021.
Data from the Office for National Statistics showed that, for the whole of 2020, there were 20 deaths in people under 19 which involved, but not necessarily were due to, Covid, whereas figures for 2021 so far show there have been 48.
“We don’t have updated data on this for the last six months, although we will in the future,” said Prof Viner. “Paediatricians across the country believe that these findings still broadly hold – that children are at extremely low risk of death from this virus.
“Most deaths of children with a positive test are not related to Covid but reflect the commonality of infection in the population, and that the children at most risk are those who have always been at higher risk – those with serious other medical conditions.”
Separate research from King’s College London had previously found that children are very unlikely to develop long Covid when compared to adults.
A study published in august found one in 20 children who catch the virus develop long Covid, with the majority making a full recovery in less than a month.
The study showed that the most common symptoms in children were headaches, tiredness, a sore throat and loss of smell.
Molly Kingsley, the co-founder of the campaign group UsForThem, told The Telegraph: “UsforThem have argued since 2020 that pandemic measures must be proportionate and non-damaging to children.
“Whilst every child death is a tragedy, this study reconfirms what we have known for a while – that the vast majority of children are at minimal risk from Covid-19.
“This raises a serious question about the appropriateness of this government’s Covid response as it applies to children – for whom school closures, mask-wearing, exam cancellation and isolation have had a devastating impact.”
Why are more people dying above what is normally observed, even after accounting for COVID-infection deaths? Doctor says Vaccines are Directly and Indirectly Killing People
/
by Dr. Joel S. Hirschhorn from [HERE] During the pandemic, many deaths have occurred in the U.S., approaching 2 million Americans. But ponder this: Have large numbers of excess deaths over pre-pandemic years resulted from something other than COVID infections?
There have been increasing articles and studies about excess deaths during the pandemic. Too many of these seem aimed at getting attention rather than being accurate and balanced.
The concept of excess deaths is simple: Deaths above what was normally observed before the pandemic. But why are more people dying even after accounting for COVID-infection deaths? Getting to the correct answer is the goal of this article.
The core issue in seeking truth is how to evaluate excess deaths during the pandemic and then explain them. If there really are non-infection excess deaths, then the goal is to rise above often bad and uncertain data from government agencies to correctly figure out whether something especially concerning is happening – perhaps something governments do not want to acknowledge and deal with, as we shall see.
Classification of deaths
To get to the truth about excess deaths it is important to make a critical distinction by defining two classes of deaths.
Class 1: First, direct pandemic effects, which are twofold.
Most attention is needed to assess the magnitude of deaths from COVID infection. These include breakthrough cases that are COVID infections despite full vaccination.
The other direct impact is deaths from COVID vaccines.
Class 2: The second class is very different. They are indirect health impacts resulting from things other than direct medical actions aimed at addressing COVID.
These are the many collateral deaths resulting from severe contagion controls used by federal and state governments, especially lockdowns, stay at home mandates, limited hospital and physician access, school closings, job losses, travel restrictions and widespread impacts on personal and medical freedom.
These many indirect impacts cause large numbers of deaths across the entire population. They are the collateral damage caused by pandemic government authoritarian actions, but not infections nor COVID vaccines. They are done, supposedly, in the name of public health.
The government does not collect comprehensive data on these indirect deaths. Be clear about this category of deaths. They are caused by all the public health systems used to address the pandemic.
To be clear, deaths directly associated with COVID infections cover a range of situations. Government agencies report COVID-related deaths. That word "related" is very important, because proving causality has been contentious. Most physicians see causality when deaths occur soon after COVID symptoms or a positive test result.
There are reasons why there are legitimate concerns and criticisms of official COVID death data. It comes down to what criteria are used to declare a death as either caused by COVID or just, in some way, related to the infection.
U.S. federal and state agencies have, for the most part, been very liberal in declaring deaths as COVID ones. This has resulted from both financial incentives, political motivations (maintaining public fear and acceptance of authoritarian government actions) and procedural government guidance.
In the latter category are guidelines from CDC for death certificates issued in March 2020 that replaced a practice used for the previous 17 years. This change allowed physicians, medical examiners and coroners to place less importance on all kinds of health problems contributing to a death and, if there was any evidence of COVID virus infection from testing (before or after death) or symptoms, to declare a death as a COVID one.
In other words, many people, especially the elderly, could have died with COVID but not fromCOVID. They may have died from their underlying medical problems and weakened immune system more than effects directly associated with COVID infection. Some die because they have been given the very expensive approved drug remdesivir that causes acute liver and kidney problems and has a death rate of over 25%. Yet their deaths go into the COVID death column.
On the other side, is the view that some people have died from COVID infection, but their deaths have not been officially declared as a COVID death. Most likely these have been people who have died at home without medical attention. It is difficult to believe that the numbers of deaths in this class could account for a large excess death figure. Why? Because people who die from COVID infection almost always experience severe symptoms as they move from stage one viral replication to stages two and three when vital organs are attacked, especially breathing problems. These typically cause them to seek medical attention, usually hospitalization where so many COVID deaths occur.
Not to be dismissed is the reality that many COVID deaths have preempted a number of normally occurring deaths, such as from the seasonal flu and many types of accidents in a more mobile population. The latter are subsumed in the COVID death data. They do not explain excess deaths. If anything, they reduce non-infection excess deaths.
Taking all this into consideration means that COVID death totals are most likely to overstate the lethality of COVID. In fact, as I have discussed elsewhere, COVID lethality for the whole population was initially overstated by Fauci to justify extreme government actions and mass vaccination. He started the pandemic by wrongly saying that the China virus was so much more deadly than the seasonal flu. Only the elderly had a high risk of death (and younger people with serious underlying medical problems) that warranted focused government attention, initially by using safe and effective generics, namely ivermectin and hydroxychloroquine, and later vaccines.
In seeking truth about excess deaths, it is most important to recognize the countless and not quantitatively reported indirect impacts of the pandemic on health and deaths of very large numbers of people who were not actually at significant risk from COVID infection.
Deaths have resulted, for example, from people not getting normal pre-pandemic health care from treatment to prevention and suffering from extreme mental stress (often pushing addiction and suicide) caused by abnormal living and negative economic conditions. Unlike direct pandemic deaths, there is hardly any useful tabulation of indirect pandemic death impacts by government agencies. In the name of public health government agencies have harmfully impacted the lives of nearly all Americans.
There is need for caution when seeing numerical excess deaths beyond official COVID deaths, in coming up with explanations that involve controversial causes. The big example is blaming what seems as major excess deaths on COVID vaccines, especially if the many indirect pandemic causes of death are not addressed, mainly because data are not readily available.
Also note that breakthrough COVID infections in fully vaccinated people that sometimes cause death are appropriately categorized as direct COVID deaths.
As I have discussed, declining vaccine effectiveness (especially for variants) make the fully vaccinated vulnerable to dying from COVID infection. But it would be wrong to say that these deaths are different than COVID ones. And wrong to place these deaths in a category of vaccine deaths. Moreover, as I have analyzed, breakthrough deaths in the U.S. most likely account for tens of thousands of deaths, much smaller than true excess deaths – though their numbers are likely to increase in coming months and years as mass vaccination continues.
For example, recently this was reported: "Former Centers for Disease Control and Prevention Director Robert Redfield said that more than 40% of people who have died from Wuhan coronavirus in the state of Maryland over the last 6-8 weeks were fully vaccinated." And government data revealed that in September, 70% of COVID-19 deaths both in Sweden and the U.K. were "fully vaccinated" individuals.
To recap, it is important to focus on the many causes of vaccine induced deaths and collateral deaths that do not result from the viral infection. Make no mistake, there are now widely recognized medical explanations of vaccine induced deaths, including a broad array of serious blood problems this author has reviewed. Data on vaccine deaths will be examined below.
Indirect health impacts
A March 2021 study examined how the pandemic caused non-infection health impacts and made it clear that they cannot be ignored:
"The COVID-19 pandemic and global efforts to contain its spread, such as stay-at-home orders and transportation shutdowns, have created new barriers to accessing healthcare, resulting in changes in service delivery and utilization globally.
"One hundred and seventy studies were included in the final analysis. Nearly half (46.5%) of them included studies focused on cardiovascular health outcomes. The main methodologies used were observational analytic and surveys. Data were drawn from individual health facilities, multicentre networks, regional registries, and national health information systems. Most studies were conducted in high-income countries with only 35.4% of studies representing low- and middle-income countries.
"Healthcare utilization for non-COVID-19 conditions has decreased almost universally, across both high- and lower-income countries. The pandemic's impact on non-COVID-19 health outcomes, particularly for chronic diseases, may take years to fully manifest and should be a topic."
A November 2020 article, "Death by Lockdown," "forecasted more than 100,000 excess deaths due to drug overdoses, suicide, alcoholism, homicide, and untreated depression – all a result not of the virus but of policies of mandatory human separation, economic downturn, business and school closures, closed medical services, and general depression that comes with a loss of freedom and choice." What was recognized is "that as bad as a virus is, policies that wreck normal social functioning will cause massive and completely unnecessary suffering and death."
A new article from the New York Post made these wise observations:
"Instead of keeping calm and carrying on, the American elite flouted the norms of governance, journalism, academic freedom – and, worst of all, science. They misled the public about the origins of the virus and the true risk it posed. Ignoring their own carefully prepared plans for a pandemic, they claimed unprecedented powers to impose untested strategies, with terrible collateral damage. We still have no convincing evidence that the lockdowns saved lives, but lots of evidence that they have already cost lives and will prove deadlier in the long run than the virus itself. A few scientists and public-health experts objected, noting that an extended lockdown was a novel strategy of unknown effectiveness. In April 2020, John Ioannidis, Jay Bhattacharya and other colleagues reported that the fatality rate among the infected was considerably lower than the assumptions used to justify lockdowns."
The TB case has been one of worst collateral health impacts of the pandemic. This was documented in a detailed story. "Tuberculosis killed roughly 1.5 million people in the first year of the COVID-19 pandemic, up from 1.4 million in 2019. And researchers say COVID is to blame." And there is every indication that it has gotten much worse worldwide.
"The COVID-19 pandemic has reversed years of progress and efforts in the fight against tuberculosis," said Dr. Tereza Kasaeva, head of WHO's global TB program. Kasaeva said that COVID lockdowns, limited access to health care and patients' concerns about visiting medical clinics made TB far more deadly during the pandemic.
Justin Hart of Rational Ground noted in October 2021 that, "It's estimated that 50% of regular child immunizations were missed in the spring of 2020. You can do some actual math, and I feel confident in saying that more children will die from missed vaccines in a year's time than died of COVID-19." This is just another example of a collateral impact of the pandemic.
The conclusion is that when examining excess deaths, it is important to recognize indirect deaths resulting from pandemic control actions by governments.
The Economist article
Here are highlights from a discussion of a widely addressed article titled "The pandemic's true death toll."
This conclusion was the attention grabber: "Fifteen million more people have died during the COVID-19 pandemic compared to historical norms, according to a recent October report by the Economist. This figure is more than three times the reported COVID-19 deaths, which stands at 4.6 million people." In other words, about 10 million excess deaths over direct COVID infection deaths.
"And what about people who died of preventable causes during the pandemic because hospitals full of COVID-19 patients could not treat them? If such cases count, they must be offset by deaths that did not occur but would have in normal times, such as those caused by flu or air pollution." These ideas fall into the class of indirect COVID impacts.
The Economist had to invoke indirect pandemic impacts in addition to vaccine induced deaths. When speaking of many millions of excess deaths globally, the only rational explanation are the widespread indirect pandemic impacts that have devastated the entire global population. This means that it has not been the virus that has killed most people, but rather government actions. It is quite plausible that for every COVID death two more people have died from the indirect impacts of pandemic management.
Here are the data reported for North America: 675,000 COVID deaths and 843,000 excess deaths (middle uncertainty). That is a very large number of excess deaths that could only be explained by health impacts of government actions. For the U.S. it was reported that the cumulative COVID-19 infection deaths have reached close to 650,000, and excess deaths are 820,000, presumably indirect deaths. Updating, for the current U.S. number of 730,000 infection deaths, that implies 921,000 indirect collateral deaths.
Important NIH and other results
Here is an important observation from a recent report from the NIH: "Roughly 2.9 million people died in the United States between March 1, 2020, and December 31, 2020. Compared with the same period in 2019, there were 477,200 excess deaths, with 74% of them due to COVID-19." That amounts to 343,584 COVID deaths during the first year of the pandemic; it is consistent with the over 730,000 COVID deaths reported since 2020.
For 2020, when COVID began ravaging the country, compared to pre-pandemic 2019, that leaves 133,616 deaths to be explained. The answer cannot be deaths associated with COVID vaccines for this pre-vaccination period. That is the key point – pre-vaccination, which means that the plausible explanation for the significant excess deaths of 133,616 are the many negative health impacts causing deaths from the expanding government pandemic control actions in 2020. These included many lockdowns, stay at home mandates, disruptions in health care and loss of jobs. In other words, collateral deaths.
In agreement with this statement was the finding in a medical journal article titled "Excess Deaths From COVID-19 and Other Causes in the US, March 1, 2020, to January 2, 2021." It said deaths attributed to COVID-19 accounted for 72.4% of U.S. excess deaths, leaving 27.6% explained most likely from collateral deaths.
A June 2021 Scientific American article said 18% of excess deaths across the U.S. last year (2020) were not assigned to COVID. Thus, 78% was related to COVID infections. Reported was that Andrew Stokes, Boston University, and his colleagues calculated excess deaths for each of more than 3,100 U.S. counties. To do so, they compared provisional 2020 mortality data from the National Center for Health Statistics with predicted death rates based on previous years. The researchers then compared the proportion of excess deaths attributed to COVID on death certificates with those assigned to other causes. Their data showed that 18% of excess deaths across the U.S. in 2020 were not assigned to COVID. That infers about 77,000 indirect deaths, reasonably explained by collateral deaths.
A journal article published in April 2021 reported: "Between March 1, 2020, and January 2, 2021, the U.S. experienced 2,801,439 deaths, 22.9% more than expected, representing 522 368 excess deaths. … Deaths attributed to COVID-19 accounted for 72.4% of U.S. excess deaths." That leaves 27.6% or a little over 144,000 non-COVID infection deaths. Detailed data were given on specific non-COVID deaths, including: heart disease, Alzheimer disease/dementia and diabetes.
A September 2021 article titled "Impact of COVID-19 on excess mortality, life expectancy, and years of life lost in the United States" found that for 2020: There were 375,235 excess deaths, with 83% attributable to direct, and 17% attributable to indirect effects of COVID-19. So, about 64,000 deaths were collateral deaths.
A new report, "Collateral Damage from COVID" said: "In the first year of the U.S. COVID pandemic (the 52 weeks ended February 27, 2021) there were 665,000 excess deaths (deaths above the normal seasonal death rate) reported by the CDC. The official COVID death toll for that span was 514,000 (77%). Shockingly, this means that non-COVID deaths caused by the pandemic and possibly by our policy choices, are likely to total at least this 151,000 difference." The latter would logically be collateral deaths.
And this is how that 151,000 difference was explained: "Excess deaths due to unnatural causes surged by an estimated 82,000 above the normal levels, from March 2020 through August 2021. Unnatural causes are dominated by homicides, suicides, overdoses, and accidents. And, excess deaths due to the Big Four natural causes (heart and lung disease, cancer, and stroke) soared by over 86,000 over those same 18 months, mostly during 2020. These two categories alone total 168,000 excess deaths." Clearly, many deaths were caused by government pandemic controls that made lives extremely difficult and stressful.
On this point, the report noted: "The death toll from unnatural causes has risen sharply and is not likely to fall as quickly. Research shows that collateral effects on health, direct and indirect, following unemployment and other economic disruption remain elevated for several years. The same seems likely to be true for overdoses and homicides, due to lingering mental health effects, though perhaps not for accidental deaths."
In contrast to the above, it was reported in October 2020 that a report by CDC said that overall, an estimated 299,028 excess deaths occurred from late January through Oct. 3, 2020, with 198,081 of them (66%) caused by COVID-19. But that left nearly three months in later 2020 unaccounted for, when COVID infections probably mounted. So, some 100,947 (or 134,596 for 12 months) excess deaths not related to COVID infection is mostly in agreement with the above figures. These CDC numbers are the least credible.
Thus, despite data variations, most of these reports were fairly consistent in attributing 72 to 83% of U.S. excess deaths over pre-pandemic years to COVID infection deaths, leaving a fairly broad range of about 64,000 to 151,000 excess deaths to non-infection causes. These would be the collateral impacts of pandemic control actions by federal and state governments, but are much lower than what The Economist estimated; but these are not systematically measured by the government.
The average of the above reports is 25.3% for non-infection deaths and for these an average of 117,745 such collateral deaths annually, and before vaccine deaths would be a significant fact.
Dr. Joseph Mercola's views
Receiving major attention on alternative news sites in October 2021 are the views of Dr. Joseph Mercola that will now be summarized. He has been a strong proponent for explaining non-infection deaths on the basis of COVID vaccines.
"The number of Americans who have died between January 2021 and August 2021 is 16% higher than 2018, the pre-COVID year with the highest all-cause mortality, and 18% higher than the average death rate between 2015 and 2019. Adjusted for population growth of about 0.6% annually, the mortality rate in 2021 is 16% above the average and 14% above the 2018 rate."
Mercola asked the key question: "Did COVID-19 raise the death toll despite mass vaccination, or are people dying at increased rates because of it?"
"The death toll from the jabs is estimated to be between 200 and 500 deaths per million doses administered. With 4 billion doses having been administered around the world, that means 800,000 to 2 million so-called 'COVID-19 deaths' may in fact be vaccine-induced deaths." This range is a high fraction of about 5 million total global COVID infection deaths. In the U.S., 414 million doses have been given; using the above range that yields a range of 82,800 to 207,000 vaccine deaths on top of the 730,000 infection deaths given by CDC.
[To be clear, vaccine-induced deaths are definitely real and significant. The issue is their magnitude. Nor is it fair to argue that vaccine induced deaths are to some degree hidden within COVID death data. And clearly it is unreasonable to argue that high COVID deaths after mass vaccination, which has been widely observed, should be counted as vaccine deaths.]
The key question is whether the high level of U.S. vaccine deaths is compatible with what the public is seeing.
Mercola also references the following:
"According to this whistleblower, the U.S. Vaccine Adverse Event Reporting System (VAERS) under-reports deaths caused by the COVID shots by a conservative factor of five or more. She claims the number of Americans killed by the shots was at least 45,000 as of July 9, 2021. At that time, VAERS reported 9,048 deaths following COVID injection. That number is now 16,310 (as of October 1, 20218). Using an under-reporting factor of five, that gives us an estimated vaccine death toll of 81,550." That is at the low end of the range calculated above.
Another source is also used by Mercola:
"Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, has come up with even more drastic numbers. In the video 'Vaccine Secrets: COVID Crisis,' he argues that VAERS can be used to determine causality, and shows how the VAERS data indicate more than 212,000 Americans have already been killed by the COVID shots." That is at the high end of the range calculated above.
To recap, Mercola's reporting provided different sources to support the range of 82,800 to 207,000 for vaccine deaths to date.
Rose and Crawford study
The September 2021 study "Government's Own Data Reveals that at Least 150,000 Probably DEAD in U.S. Following COVID-19 Vaccines," by Jessica Rose and Mathew Crawford, is the most detailed and impressive effort to determine vaccine deaths. It has been criticized by FDA: "Although under reporting is a limitation in VAERS, with regard to COVID-19 vaccine safety monitoring, there currently is not evidence to suggest it would underestimate the amount of COVID-19 vaccine-related deaths to such a large degree." This author disagrees with FDA. Here is the official view of CDC: "'Underreporting' is one of the main limitations of passive surveillance systems, including VAERS. The term, underreporting refers to the fact that VAERS receives reports for only a small fraction of actual adverse events." As you will see below, the 150,000 figure for vaccine deaths is a low, conservative estimate.
This is the summary of its findings: "Analysis of the Vaccine Adverse Event Reporting System (VAERS) database can be used to estimate the number of excess deaths caused by the COVID vaccines. A simple analysis shows that it is likely that over 150,000 Americans have been killed by the current COVID vaccines as of Aug 28, 2021." This is close to the high end of the range given above.
The study is both long and complex. Here are some highlights.
On the problem of underreporting of vaccine deaths: "In our informal physician surveys we saw a bias to under-report serious adverse events in order to make the vaccines look as safe as possible to the American public since most physicians believe they are hurting society if they do anything to create vaccine hesitancy. Secondly, we'd estimate that at least 95% of physicians have completely bought into the "safe and effective" narrative and thus any event that they observe they deem as simply anecdotal and don't bother to report it since it couldn't have been caused by such a safe vaccine that appeared to do so well in the Phase 3 trials."
On the search for quantifying underreporting in the CDC VEARS system: "The point of this paper is not to find the exact number of deaths, but merely to find the most credible estimate for deaths. We think that anaphylaxis is an excellent proxy for a serious adverse event that, like a death, should always be reported so we think 41X is the most accurate number." That means multiplying CDC numbers by 41.
To get estimates of vaccine deaths: "There are three ways to estimate the number of excess deaths caused by the vaccine. Using these three methods we can estimate the low and high likely bounds for the number of excess deaths caused by the vaccine:
1. Subtract the average number of background deaths in previous years: estimate is 252,109;
2. Use 86% based on the analysis in the Mclachlan study; estimate is 252,073;
3. Use 40% based on the estimate of Dr. Peter Schirmacher one of the world's top pathologists; estimate is 175,865."
This was the explanation for looking at other studies: "In order to validate that our estimates are reasonable (or simply that the evidence was more likely consistent with the hypothesis that the vaccine does more harm than good), we looked at four different quantitative methods from very small to very large and summarized their estimates:"
Excess Case Fatality Rate analysis done in Europe: 72,000-180,000
Excess death analysis for 23 nations: 147,960
Small island study: 171,000
Analysis of Norway deaths: 150,000
"In summary, the qualitative and quantitative confirmation techniques we used were all independent of each other and of our main method, yet all were consistent with the hypothesis that the vaccines cause large numbers of serious adverse events and excess deaths and are inconsistent with the null hypothesis that the vaccines have no effect on mortality and have a safety profile comparable to that of other vaccines."
"We were not able to find a single piece of evidence that supported the FDA and CDC position that all the excess deaths were simply over-reporting of natural cause deaths."
In wrapping up a very complex analysis this was said:
"In 1976, they halted the H1N1 vaccine after 500 GBS cases and 32 people died. However, there is no stopping mortality condition for these [COVID] vaccines. We are likely at 150,000 deaths and counting and nobody in the mainstream medical establishment, mainstream media, or Congress is raising any concerns. No member of the medical community is calling for any stopping condition nor autopsies. We find this troubling."
Here is the most important reason for respecting this study. As you can see the final estimate of 150,000 vaccine deaths is lower than other figures in various studies but consistent with the range from Mercola's reporting. Overall, this figure of 150,000 vaccine deaths is conservative.
Here are more concluding insights that the public should greatly think through, especially when deciding whether or not to get a vaccine shot, initial or booster:
"In short, say our vaccine reduces the risk of dying from COVID by 2X. But it came at a cost, e.g., increasing your risk of dying from a heart attack by 4X. And let's say both events are equally likely (which they aren't). Then you've made a bad decision … you're more likely to die if you took the vaccine.
"When you combine (1) the negative efficacy of the vaccine with (2) the negative all-cause mortality benefit, it's impossible to justify vaccination. Either alone is sufficient to kill the benefit; both of them together makes things even more difficult for recommending vaccination.
"The bottom line is clear: If you got the vaccine, you were simply more likely to die. The younger you are, the greater the disparity."
As more Americans succumb to pressure, propaganda and mandates, it is very likely that the figure of 150,000 vaccine deaths will become an underestimate of the lethality of COVID vaccines.
Lastly, it is relevant to note what the eminent medical researcher Dr. Judy Mikovits has said. Her medical science credentials are impeccable, including a long stint at the National Cancer Institute. Her views may seem extreme to some people, but they are based on a deep scientific understanding and are consistent with the highly frightening forecasts of other scientists and physicians.
She said: "I just can't even imagine a recipe for anything other than what I would consider mass murder on a scale where 50 million people will die in America from the vaccine." Time will tell whether this dire prediction will materialize as more people get the shot. The shot that kills.
Israel deaths
Since the start of the third booster shot on July 30, the COVID death rate in Israel has been reported to have jumped from about .15 to 3.5 per million in early September. Is it possible that a similar negative impact will happen in the U.S.?
In an August 2021 paper entitled "Young adult mortality in Israel during the COVID-19 crisis,"noted Israeli researcher Dr. Steve Ohana examined a surge in Israeli youth deaths, which he says are unexplained by anything other than a surge in vaccinations for the age group 20-49." Specifically, he noted that, "the surge in mortality coincided with the rollout of the Israeli vaccination campaign for the 20 s to 49-year-olds, which reached more than 75% of individuals in this age group." Dr. Ohana concluded that his findings should "urgently prompt a pause in the vaccination campaign, until the reasons of the youth excess mortality observed in mass vaccination countries are clarified."
Finally, here is perhaps the most interesting development in Israel recently reported. "There are a million people that are currently about to surrender their freedoms instead of getting a booster." This means that 1 million people in the most vaccinated country on the planet were letting their Green Pass expire." This would greatly curtail their freedom to access many places.
A report from Israel examined excess deaths for one period and reported the following: "According to data from the Central Bureau of Statistics (CBS), during January-February 2021, in the midst of the vaccination operation, there was a 22% increase in overall mortality in Israel compared to the bi-monthly average mortality in the previous (pre-vaccination) year. In fact, the period of January-February 2021 is the deadliest one in the last decade, with the highest overall mortality rates, when compared to the corresponding months over the last 10 years. The report highlights that younger people between the ages of 20-29 appear to be the demographic that saw the most dramatic increase in mortality following the rollout of the Pfizer vaccine. In this group, during the same vaccination period, January-February 2021, there has been a 32% increase in overall mortality compared to the bi-monthly average mortality in 2020."
As the U.S. pushes booster shots for everyone, including young people, there may be lessons to learn from Israel.
Conclusions
It is challenging to reconcile the average of 117,745 excess deaths beyond infection deaths given above with the conservative figure of 150,000 vaccine deaths. Add in the indirect, even higher collateral deaths across society broadly, probably what The Economist found, namely for the current U.S. 730,000 infection deaths and some 921,000 indirect collateral deaths. The latter seems reasonable when you consider that most of the population, several hundred million people, had their lives devastated by government pandemic controls. In other words, a collateral death rate of around .5%.
As to the latter, though taken in the name of public health, most government actions have had no basis in medical science. Considering all the deaths, pandemic management has been a colossal failure with the highest level of COVID infection deaths globally in the U.S.
Adding up the infection, vaccine and collateral deaths gets to a total approaching 2 million pandemic deaths. And note that breakthrough infections of the fully vaccinated are escalating, as vaccines lose effectiveness, and are at least 10,000 to 20,000.
Public health officials failed to promote early wide use of generics and foolishly pushed mass vaccination that has not proven effective. The former could have prevented over 600,000 infection deaths.
Perhaps the greatest tragedy is that public health officials have stubbornly refused to admit their mistakes.
The government has made no attempt to systematically account for the non-infection indirect collateral pandemic deaths. And surely more and more Americans are dying from the onerous pandemic controls – now emphasizing vaccine mandates – that are destroying and disrupting the lives of millions of people. Especially in view of the above estimates for vaccine deaths.
Finally, and most importantly, nearly all of the excess deaths approaching 2 million Americans could have been prevented by better government policies:
1. COVID infection deaths could have been prevented by promoting wide use of a number of protocols to cure and prevent infection by using generic medicines and other proven drugs. And also by aggressive programs to address obesity, diabetes and various causes of weakened immune systems.
2. Vaccine deaths could have been prevented by focusing on about 5% of the population at significant risk from fatal COVID but not the entire population, meaning no vaccine mandates.
3. Not using invasive contagion controls, namely lockdowns, that have disrupted and destroyed lives and caused huge numbers of collateral deaths.
Dr Asks 'If hospitalizations/deaths are almost exclusively occurring in the UnVaxed why would booster shots be necessary? Why are most COVID hospitalizations/deaths in the UK among the Fully Vaxxed?'
/From [HERE] U.S. Sen. Ron Johnson (R-Wis.) Tuesday held a roundtable discussion on federal COVID vaccine mandates with a panel of people injured by COVID vaccines and scientists from some of the most prestigious research organizations in the world, including The BMJ and Massachusetts Institute of Technology (MIT).
Peter Doshi, a senior editor at The BMJ and associate professor of pharmaceutical health services research at the University of Maryland School of Pharmacy, and Retsef Levi, a health system and analytics professor at MIT, expressed doubts about COVID vaccine efficacy and the failures of the scientific community.
“I’m saddened we’re super-saturated as a society right now in the attitude of ‘everybody knows,’ which has shut down intellectual curiosity and led to self-censorship,” said Doshi.
Doshi said we’re not in a “pandemic of the unvaccinated.” If hospitalizations and deaths are almost exclusively occuring in the unvaccinated “why would booster shots be necessary?” Doshi asked. “And why would the statistics be so different in the UK, where most COVID hospitalizations and deaths are among the fully vaccinated?”
“There’s a disconnect there, and something to be curious about,” Doshi said. “There’s something not adding up.”
Doshi argued the public was lied to in early 2021, when health officials including Dr. Anthony Fauci, claimed COVID vaccine trial data proved the vaccine saved lives.
After presenting the trial data for the vaccines authorized for use in the U.S., Doshi pointed out “there were similar numbers in the vaccine and placebo groups.” He argued those “who claimed the trial showed the vaccine was highly effective in saving lives were wrong” and that “the trials did not demonstrate this.”


Doshi talked about anti-vaxxers and criticized the official definition of the term. He presented the panel the official Merriam-Webster definition of anti-vaxxer: “A person who opposes the use of vaccines or regulations mandating vaccination.”
“The second part [of the definition] stunned me,” said Doshi.
“There are entire countries from the United Kingdom to Japan which do not mandate childhood vaccines,” he said. “There are no mandates, and I would wager that perhaps a majority of the world’s population meet this definition of an anti-vaxxer.”
Doshi told the panel that “vaccine” is another definition “worth checking on.”
“I argue these products which everyone calls MRNA vaccines are qualitatively different from standard vaccines,” Doshi said. “So I found it fascinating to learn that Merriam Webster changed the definition of vaccine early this year.”
“mRNA products did not meet the definition of vaccine that has been in place for over 15 years, but the definition was expanded such that mRNA products are now vaccines,” Doshi said.
He then argued that just because we’re calling the COVID shot a “vaccine” doesn’t mean “these new products are just like all other childhood vaccines which get mandated.”
“Each product is a different product, and if people are OK with mandating something simply because it’s a vaccine, I believe it’s time to inject some critical thinking into the conversation,” Doshi said.
He also criticized the fact that society is vaccinating and mandating the vaccine for large portions of the public despite the raw data on the safety and efficacy of the vaccines not being available yet.
“So while we are told to keep following the science, what we are following is not a scientific process based on open data, we are following a process where the data are secret, and in my view there is something very unscientific about that,” Doshi said.
Levi told the panel “scientists in the most prestigious journals assert that the vaccine is safe, failing to report on serious side effects such as deaths.”
He explained that national emergency services calls in Israel for cardiac arrest among young individuals under 40 years old saw a dramatic increase — more than 25% — in parallel to the COVD vaccination campaign.
“We wrote an academic paper raising concerns regarding these statistics and called on the authorities to check on this … needless to say they never got back to us.”
Levi claimed the government attempted to censor the research by calling its credibility into question. “They called the research fake,” Levi said.
Levi warned the panel:
“These vaccines have serious and unknown side effects, and we need to use them with caution.” [MORE]
Pandemic of the Vaccinated? Contrary to Government Lies, Data from 188 Countries Proves the Highest COVID Case Rates are in the Most Vaccinated Countries
/From [theExpose] Worldwide analysis of 188 nations shows a massive global correlation between vaccination and higher case rates of Covid-19, proving the world is currently experiencing a pandemic of the vaccinated.
METHOD
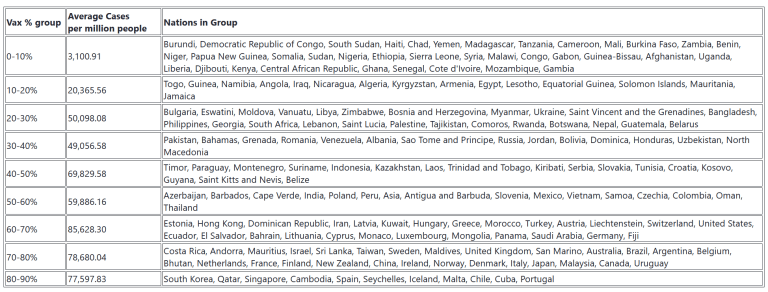
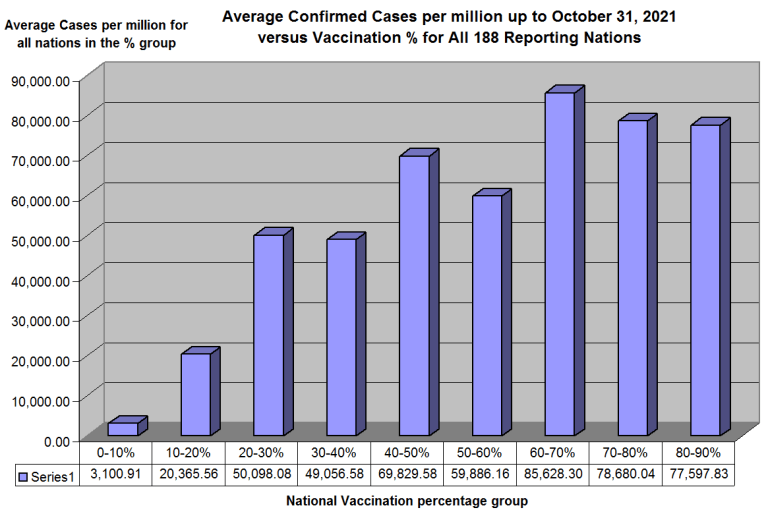
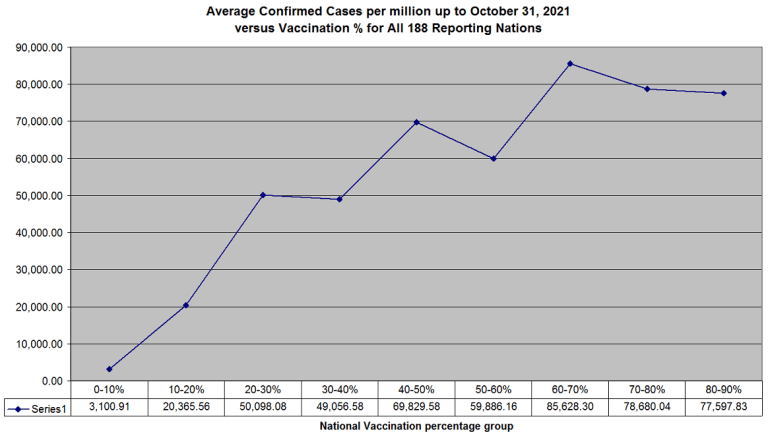
Data was analysed from the ‘Our World in Data’ site of Johns Hopkins University on 247 million Covid-19 cases from the very start of the pandemic to October 31st 2021, for all 188 nations where they have data on both the percentage of people vaccinated and the cumulative confirmed cases per million .
The results on the average cases per million people against the percentage vaccinated were as follows –
CONCLUSION
The above shows that the incidence of cases increases fairly linearly with the percentage of vaccinated people at a rate of 800 cases per million per extra percentage vaccinated.
The nations with the lowest case rates are almost exclusively in Africa, which also has the lowest rates of vaccination.
Whereas the nations with the highest case rates also have the highest rates of vaccination.
The inescapable conclusion from all the data we have up to October 31st is that vaccines increase case numbers. This is not a representative sample of a few thousand cases from one nation. It is a full study of all the cases so far in every reporting nation.
The results are in. There is a massive correlation positive between vaccination percentage and case numbers. Vaccinations are clearly opening the door to the virus.
In heavily vaccinated nations such as the UK the case rate in the fully vaccinated over 30’s is presently only 23-55% higher than the case rate in the unvaccinated. But the case rate in the unvaccinated is elevated due to infection by vaccinated people.
The media narrative is that the unvaccinated are infecting the vaccinated. This data indisputably shows that the reverse is the case. This has now become a pandemic of the vaccinated.
They are increasing the case numbers in the unvaccinated – because their immune systems are being damaged by the vaccines. That is what the fairly straight and very steep line above is declaring.
Had there been no vaccination in the UK the figures would now be more like those of the African countries as seen in the bottom left of the above graph.
One of the clearest ways to see that the vaccinated are infecting the unvaccinated is the comparison of 71% vaccinated in Israel with 27% vaccinated in Palestine.
The graph shows Israel leading Palestine in cases and dragging them up above the world average case level.
More than Half of US States are Suing to Stop the Blight House COVID Vaccine Mandate
/
From [HERE] More than half of U.S. states are suing to stop the Biden administration from implementing new rules that require employers with more than 100 workers to ensure their employees are vaccinated against Covid-19 or get a weekly test.
The states’ attorneys general, who filed multiple lawsuits in various courts Friday, said they were suing because the federal government doesn’t have the authority to issue the requirements. They say the issue should be left to states.
“States have been leading the fight against COVID-19 from the start of the pandemic,” Kansas Gov. Laura Kelly, a Democrat, said Friday. “It is too late to impose a federal standard now that we have already developed systems and strategies that are tailored for our specific needs.”
In September, Nina Pierpont (MD, PhD) published a paper on September 9th, entitled “Covid-19 Vaccine Mandates Are Now Pointless: Covid-19 vaccines do not keep people from catching the prevailing Delta variant and passing it to others.” It analyzes 3 major studies published in August 2021 which together demonstrate the COVID injections do not prevent infection or transmission of Covid-19. As such, she concludes that vaccine mandates are unjustified and baseless.
Dr. Pierpoint is a graduate of Yale University (BA in biology), with a MA and PhD from Princeton University in population biology/evolutionary biology/ecology, and the MD degree from the Johns Hopkins University School of Medicine. She has been a Clinical Assistant Professor of Pediatrics at Columbia University’s College of Physicians & Surgeons. She is currently in private practice in upstate New York, specializing in behavioral medicine.
The paper states the following:
“Executive Summary:
1) Excellent scientific research papers published or posted in August 2021 clearly demonstrate that current vaccines do not prevent transmission of SARS-CoV-2.
2) Vaccines aim to achieve two ends:
a. To protect the vaccinated person against the illness.
b. To keep people from carrying the infection and transmitting it to others.
i. If enough people are vaccinated or otherwise become immune, it is hoped that the disease will stop circulating. We call this herd immunity.
ii. On the way to herd immunity, there is an assumption that people who are immunized can form safe clusters or groups within which no one is carrying or transmitting the virus.
3) Unfortunately, this last assumption (2.b.ii) is no longer true under the new variant of SARS-CoV- 2, Delta (B.1.617.2), which now accounts for essentially all cases worldwide.
4) Delta is more infectious than the Alpha strain (B.1.1.7) that prevailed in the UK from January to May 2021 (and in the US from March to June 2021), meaning that Delta is passed more readily person-to-person than the previous dominant strain.
a. Infectiousness is a correlate of high viral load (see section 5, below).
b. From its origin in India, Delta has soared to nearly complete domination of COVID-19 viral strains everywhere in a matter of months, because it spreads so easily and infects both vaccinated and unvaccinated people.
5) New research in multiple settings shows that Delta produces very high viral loads (meaning, the density of virus on a nasopharyngeal swab as interpreted from PCR cycle threshold numbers).
a. Viral loads are much higher in people infected with Delta than they were in people infected with Alpha.
b. Viral loads with Delta are equally high whether the person has been vaccinated or not.
c. Viral load is an indicator of infectiousness. [13,14] The more virus one has in the nose and mouth, the more likely it is to be in this individual's respiratory droplets and secretions, and to spread to others.
6) Due to evolution of the virus itself, all the currently licensed vaccines (all based on the original Wuhan strain spike protein sequence) have lost their ability to accomplish vaccine purpose 2(b), above, "To keep people from carrying the infection and transmitting it to others."
7) Vaccine mandates are thus stripped of their justification, since to vaccinate an individual no longer stops or even slows his ability to acquire and transmit the virus to others.
8) Under Delta, natural immunity is much more protective than vaccination. All severities of COVID-19 illness produce healthy levels of natural immunity. [MORE]
Surgeon General Disrupts NFL Pre-Game to Remind Unmasked Fans, 'Biden's Dictates Good: Mandates are Necessary Even Though Vaccines Don’t Prevent COVID, Stop its Spread and May Harm or Kill You'
/

From [HERE] U.S. Surgeon General Dr. Vivek Murthy defended the actions of the Biden administration in a Sunday interview on ABC's "This Week" after it announced a sweeping COVID-19 vaccine mandate for companies with 100 employees or more.
"The president and the administration wouldn't have put these requirements in place if they didn’t think that they were appropriate and necessary, and the administration is certainly prepared to defend them," Murthy told ABC News "This Week" co-anchor Martha Raddatz, adding that the U.S. has a history of using vaccine requirements to protect the population.
The Biden administration on Thursday released new federal rules that view COVID-19 as an occupational hazard, meaning nearly 100 million U.S. workers will be required to have proof of the COVID-19 vaccine by Jan. 4, with some workers allowed to test weekly.
"It's important we take every measure possible to make our workplaces safer," Murthy said. "It's good for people's health, it's good for the economy, and that's why these requirements make so much sense." [MORE]

Reports Show 3 More Teens Died After Getting Injected w/COVID Vaccines, as Reported Injuries Exceed 850,000
/
From [HERE] Data released today by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020, and Oct. 29, 2021, a total of 856,919 adverse events following COVID vaccines were reported to the Vaccine Adverse Event Reporting System (VAERS).
The data included a total of 18,078 reports of deaths — an increase of 459 over the previous week. There were 127,457 reports of serious injuries, including deaths, during the same time period — up 3,570 compared with the previous week.
Excluding “foreign reports” to VAERS, 634,609 adverse events, including 8,284 deaths and 52,685 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Oct. 29, 2021.
Of the 8,284 U.S. deaths reported as of Oct. 29, 10% occurred within 24 hours of vaccination, 15% occurred within 48 hours of vaccination and 26% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 418.6 million COVID vaccine doses had been administered as of Oct. 29. This includes: 246 million doses of Pfizer, 157 million doses of Moderna and 15 million doses of Johnson & Johnson (J&J). [MORE]
Is the US Response to COVID an Official Government Psychological Operation? “Biocide?"
/From [HERE] “Where, after all, do universal human rights begin? In small places, close to home — so close and so small that they cannot be seen on any maps of the world. Yet they are the world of the individual person; the neighborhood he lives in; the school or college he attends; the factory, farm, or office where he works. Such are the places where every man, woman, and child seeks equal justice, equal opportunity, equal dignity without discrimination. Unless these rights have meaning there, they have little meaning anywhere. Without concerted citizen action to uphold them close to home, we shall look in vain for progress in the larger world.” — Eleanor Roosevelt
Those who have questioned the intentions behind government policy in response to the pandemic continue to observe the unreasonable intensity of supporters of mandated protocols. Declaring vehement loyalty to vaccine therapy, their minds are closed to any further input.
Vaccination proponents don’t want to see or hear anything contradicting their very confident, though most questionable position: that a benevolent government, supported by a monolithic, knowledgeable, scientific community, is successfully dealing with the crisis.
In addition to the challenges of an uncompromising public debate, some of us face a personal crisis: The compassionate principles of long-term relationships are being tested.
With entrenched devotion to vaccines, loved ones and friends who were once willing to discuss most other topics, refuse to engage. At a minimum, they express disappointment in our lack of understanding and compliance. When forthright they confess their judgment — our unwillingness to conform causes continuing affliction.
Many people have been persuaded that anyone who has doubts about the infallible words and irrefutable facts presented by somber leaders and an impartial press corps are infecting others with dangerous information.
Failures of the pandemic response are increasingly laid at the feet of the unvaccinated.
However, the furious indignation is often irrational, inordinate and out of character, suggesting it is driven by a set of external stimuli designed to create the response.
A looming crisis, initially presented with expectations of horrific consequences including widespread severe disease and millions dead, can be viewed as the beginning of a prescribed government response to the pandemic.
The intentional amplification of the threat, unjustifiable by any scientific defense, was never diminished, even as ominous predictions of suffering and mortality proved to be greatly exaggerated.
From the moment vaccines were released, anyone who doubted their importance and efficacy has been depicted as a hostile deviant entranced by fantasies or blindly following aberrant leaders.
And although so-called anti-vaxxers are belittled for their ignorance, there is no indication those rejecting enforced protocols are doing anything but defending their inalienable rights — life, liberty and the pursuit of happiness.
The extreme aggressive tactics of the government and media to promote vaccines — including a campaign to humiliate those who refuse to comply — have the earmarks of psychological warfare, with manipulation of citizens on a grander scale than any effort in recent history.
The continuing prevailing mindset of many people appears to be the reaction to a calculated induction of a mass hypnotic trance.
Of all aspects of pandemic response, this is one of the most troubling, and should cause us to consider its probability, provenance and rectification.

‘My honor is my loyalty’
The government’s use of a psychological operation — aka PSYOP — to promote immunization follows standards and practices for engendering a cult mentality to reach its objectives.
The central technique for initiating and maintaining an obedient population is developing an “us versus them” mindset. The demonization of outsiders is essential.
Demands and sacrifices are made of the members, solidifying their involvement and ensuring they see themselves as superior to those who don’t participate.
These mesmeric psychological operations can be identified in groups small and large, including mass populations.
The most dramatic example of a PSYOP engendering a cult is the rise of fascism in Nazi Germany. An elite propaganda machine entranced a nation into believing they were a superior race, arousing a blind loyalty to their cause, with a loss of moral parameters unmatched in modern history.
Hitler’s most loyal troops, the SS, closely associated with forced labor and death camps, and deemed a criminal organization by the Nuremberg tribunals, wore belt buckles and kept daggers engraved with the words, “my honor is loyalty.”
More recently, less-militarized cults have made some dramatic impact in the United States.
The religious organization, the People’s Temple, in its early days gained the support of politicians and manipulated the media to project a positive spin on its activities.
The People’s Temple devolved into darkness, eventually leading to a quintessential cult event in Jonestown, Guyana. On the cusp of being arrested for the murder of a visiting congressman, their leader, Jim Jones, demanded the highest level of loyalty: Hundreds of members committed mass suicide, including their children, by drinking a cyanide-valium cocktail.
Mass hypnosis allows transference of an individual’s attention and priorities to a singular objective or ideology, and loyalty to the cause is elevated, overshadowing self-preservation.
Another example of an influential cult based in the United States is the Unification Church. Their members, the Moonies, were staunchly loyal to Sun Myung Moon, who was famous for presiding over spectacular mass weddings of arranged marriages.
The Unification Church also funneled money to powerful politicians through grants and speaking fees. Moon founded the Washington Times, which openly supported his political agenda.
As a lead investigator in a BBC biography of the Korean Cult leader, I met and interviewed former devotees and abettors who described the process of indoctrination into a trance of blind obedience.
Moon created a sophisticated psychological framework to attract and retain members, claiming he was a messiah greater than Buddha, Jesus and Mohammed combined. Good-hearted, intelligent people succumbed to a psychotic euphoria invoked by Moon and his agents, with support from government and media.
Only later did they awaken to their profound mistake, falling for rhetoric they eventually recognized as hypnotic, deeply flawed and dangerous.
One of the interviewees spoke most eloquently about having lost his soul, and given away years of his life.
An individual whose attitude embraces the affirmation — “my honor is loyalty” — towards any leader, cult or policy, has given up his or her personal power, often to abusive forces.
Symbolically, the SS motto has been illegal to use in Germany since 1947.
Cults are often viewed as aberrations that occurred in the past, however, they continue to thrive.
The susceptibility of humans to mass hypnosis and manipulation continues to be exploited and has never been applied for the greater good.
Cult of the vaccinated
Those who resist vaccination are reacting to harsh directives and overt hostility from a heavy-handed government. Their position is neither the result of mass hypnosis nor cult-like programming, rather an exercise in freedom of speech and choice.
Psychologically, there is an indisputable, definitive metric that demonstrates the difference between the anti- and pro-vaccine groups.
A large majority of the unvaccinated have reviewed information and statistics from a range of sources, that either support or contradict government policy. They have made choices based on concerns about efficacy and risks, but are open to engaging in debate.
Most of the pro-vaccine faction stand by what they deem unassailable information from the news media. They are willing to accept a filtered version of data, and staunchly refuse to look at any material that might cause doubt about their decisions or challenge authoritative mandates.
They refuse to engage in debate.
A majority of the general public has been beguiled into feeling threatened by the virus, and roused to angrily denounce those who doubt the efficacy or risks of COVID-19 inoculants.
The pro-vaccine disciple’s lockstep, cult-like behavior is classic. The mentality includes:
Unbending loyalty to a methodology promulgated by influential leaders who make claims that are too good to be true.
Unquestioning adherence to and dependency on the group’s approach and procedures, with insistence that they are on the only true and worthy path.
Unwillingness to consider any written or spoken words, or ideas that counter the messaging of leaders or the group’s intentions.
Willingness to change lifestyle or engage in risky behavior, with blind acceptance that there are only benefits and minimal risks.
Continuing belief in dogma, even when firmly presented concepts devolve, or prove to be deeply flawed.
Denying any self-doubt in the name of a greater mission — critical thinking about the group is an abomination.
Persuading or pressuring new members to join, using guilt as primary motivation. When this fails, forcing submission through ridicule, mental anguish or material punishment.
Demeaning, isolating and penalizing anyone who defects or does not enlist.
Willingness to dishonor family or destroy long-term relationships in the name of the cult’s objectives.
Self-destructive behavior — as in all of the above — that eventually leads to dissolution of the cult and irreparable harm to the members.
Designing a PSYOP for a pandemic
A strong circumstantial case can be made that there is an imposed PSYOP in place in the United States. The vehement public support and willingness to obey without question are the precise results a government would seek in response to the perceived threat of a deadly pandemic.
The tactics used to generate this kind of outcome are not hidden from those willing to consider how the U.S. government applies its knowledge.
This excerpt from the opening chapter of the “U.S. Army Field Manual on PSYOP” makes intentions of a campaign very clear: [MORE]
Shelter in Place Orders and COVID Job Loss are Not Legal Defenses for Failure to Pay Yurugu's Rent in Yurugu's Courts. Evictions Mount as MD, Other States Fail to Distribute 30% of Rent Assistance
/
From [HERE] Maryland missed a federal bench mark for distributing millions of dollars in emergency assistance to help tenants pay their rent, the Treasury Department told a U.S. senator, drawing a warning from the agency.
The department said in an Oct. 26 email to Sen. Chris Van Hollen that Maryland is among the states that could lose some of the funding because it failed to spend 30% of the money by Sept. 30.
“As you know, Maryland is one of the states that may be subject to reallocation because it is below the 30% expenditure ratio,” said the email, which was obtained by The Baltimore Sun.
Van Hollen and fellow Democratic Maryland senator Ben Cardin sent a letter on Friday to Kenneth Holt, secretary of the state Department of Housing & Community Development, urging the agency to speed up the disbursement of the money, which is intended to help renters avoid eviction during the pandemic.
The state needs to act quickly “to avoid having these funds revoked by the Treasury Department beginning on November 15th, leaving tens of thousands of vulnerable Marylanders needlessly at risk of losing their homes,” the letter said.
Many other states or territories have also not moved as quickly as Treasury had hoped. According to Treasury data, about three-fifths of the states joined Maryland in not meeting the initial timeline.
The Treasury Department has told states that they needed to have spent 30% — Maryland’s figure was between 25% and 30% — or have allocated at least 65% of the funds by the end of September. It said it would begin reallocating states’ unspent money in mid-November unless remedial action was taken.
Mike Ricci, a spokesman for Republican Gov. Larry Hogan, told The Sun: “The state is not at any risk of reallocation of funds, and it is false to claim otherwise.” He accused Van Hollen of not doing his “homework.”
The Treasury Department recently told states there are a few ways for states to avoid or mitigate losing funds, including submitting “program improvement” plans detailing their approaches. A Treasury spokesperson declined to respond Friday to questions from The Sun specifically about Maryland’s situation.
Ricci cited forecasts from the Department of Housing & Community Development to demonstrate the state’s progress.
“Based on the department’s projections, the October report will reflect that the state has more than exceeded Treasury’s targets,” Ricci said. “We have said all along that we are well on track to exceed those targets.”
Maryland launched its Emergency Rental Assistance Program in May 2020 with the help of $401 million in federal money approved for pandemic relief. About $143 million of that pot was divided among the state’s eight largest jurisdictions, including Baltimore City, while the remaining money was allocated to the Department of Housing & Community Development for statewide distribution.
The money was intended to help state residents at risk of losing their homes. State eviction protections expired on Aug. 15 and a federal eviction moratorium expired at the end of that same month.
In their letter, Van Hollen and Cardin noted that several surrounding jurisdictions, including Virginia, Pennsylvania and Washington, D.C., have spent larger portions of their funding than Maryland, “as have all local government grantees.”
The senators cited Anne Arundel County (74%), Baltimore City (85%), Frederick County (71%), and Prince George’s County (88%).
In August, Ricci chided local government officials, particularly Baltimore City, for their slow pace in distributing money.
Vaccine Injured Speak Out at US Senate Panel on COVID Vaccine Injuries and Deaths while Dependent Media Continues to Make [us] Believe Vax is Safe and it Stops the Spread and Transmission of COVID
/THE ELITES AT YOUTUBE, VIMEO AND FAKEBOOK REMOVED THE VIDEO BELOW; VIDEO OF A SENATE HEARING. REAL RADICAL STUFF (please check it out for yourself). SAID ELITES ARE LIARS COMPLICIT IN GENOCIDE

From [HERE] U.S. Sen. Ron Johnson (R-Wis.) on Tuesday held a discussion with a panel of experts, including clinicians, scientists, lawyers and patient advocates, and with people injured by COVID vaccines, who gave powerful testimonies about their experiences.
Johnson and the expert panel discussed the importance of early treatment for COVID, healthcare freedom and natural immunity, the impacts of mandates on the American workforce and the economy, COVID vaccine safety concerns and the lack of transparency from federal health agencies in response to his COVID oversight requests.
None of the major mainstream media outlets picked up the event, but Children’s Health Defensehosted Johnson’s live panel discussion on CHD.TV.
Cody Flint [57.20], a 33-year-old airline pilot from Cleveland, Mississippi, was among those who spoke out about their injuries. Flint was healthy and had no underlying health conditions prior to receiving Pfizer’s COVID vaccine.
Within 30 minutes of getting his first dose on Feb. 1, Flint developed a severe stabbing headache that later became a burning sensation in the back of his neck.
Two days later, he got into his airplane to do a job and quickly realized something wasn’t right.
Flint explained:
“I was starting to develop tunnel vision and my headache was getting worse. Approximately two hours into my flying I pulled my airplane up to turn around and felt an extreme burst of pressure in my ears. Instantly I was nearly blacked out, dizzy, disoriented, nauseous and shaking uncontrollably. By the grace of God I was able to land my plane without incident, though I do not remember doing this.
“My initial diagnosis of vertigo and a severe panic attack — although I’ve never had a history of either of these — was later replaced with left and right perilymphatic fistula, eustachian tube dysfunction and elevated intracranial pressure due to brain swelling. My condition continued to decline and my doctors told me only an adverse reaction to the Pfizer vaccination or major head trauma could have caused this much spontaneous damage.”
Flint underwent numerous spinal taps and two surgeries to address the fistulas and intracranial pressure. He said he has more questions than answers, does not know if he will ever be able to fly a plane again, lost a year of his life and part of his children’s lives.
“This vaccine has taken my career from me, and the future I have worked so hard to build,” Flint said. “I used all my savings just to pay medical bills just to be able to survive. My family is on the verge of losing everything we have.”
Flint, who is pro-science and pro-vaccine, said the main issue rests squarely on the fact that the U.S. Food and Drug Administration (FDA), Centers for Disease Control and Prevention (CDC) and NIH (National Institutes of Health) refuse to acknowledge that real lives are being absolutely destroyed by this vaccine.
“The federal government has yet to help a single one of the vaccine-injured,” Flint said. “It was my understanding the federal government accepted the responsibility of helping people injured by vaccines, considering they gave pharmaceutical companies fully legal immunity from people like me.”
Flint said it is time for the government to stop silencing vaccine injuries like his, and it is unconscionable for these agencies not to help.
Lt. Col. Theresa Long [101:00], a U.S. Army surgeon, said she believes the COVID vaccine is a greater threat to a soldier’s health and military readiness than the virus itself.
“Over 200,000 service members have rejected the vaccine yet the military is pressing forward without regard to the damage to the morale and readiness to process these soldiers out,” Long said. “We have never lost 200,000 soldiers on the battlefield in a few months. Taking soldiers out of uniform has the same impact on readiness as losing them on the battlefield.”
Long explained she tried to get senior leadership within the military to inform military members of the risks of vaccines, as required by informed consent.
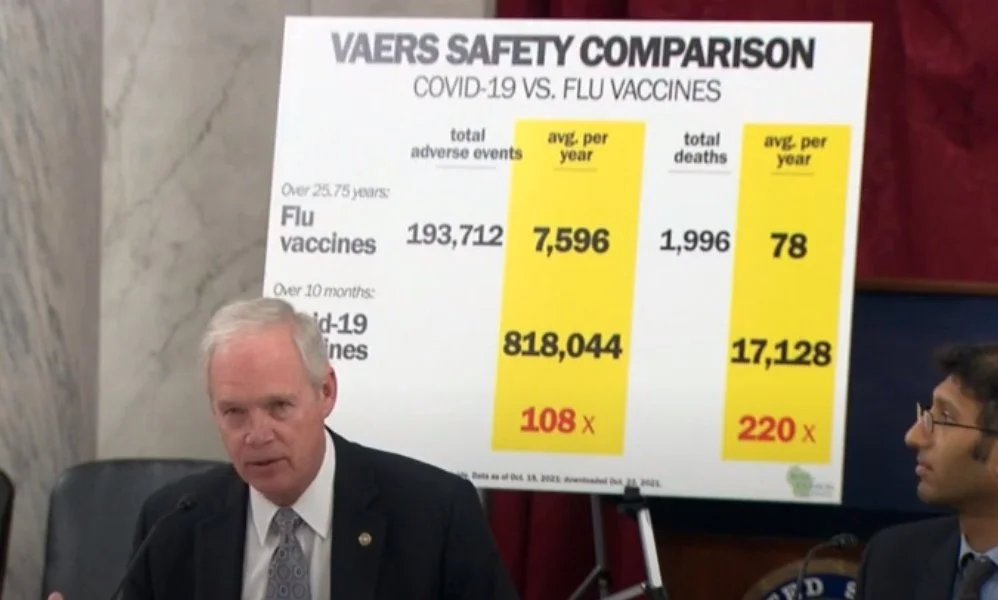
Tech Philanthropist says Governments and Dependent Media Are Lying About COVID Vax Safety; "Vaccines" are Killing 15 People for Every 1 life They Save
/
From [HERE] According to Steve Kirsch, The CDC and the FDA claim that we can safely ignore the huge spike in event rates reported to the VAERS system this year (this is the official adverse event reporting system relied on by the FDA and CDC to spot safety signals). In their view, there is “nothing to see” in the death chart below. They claim that the propensity to report (PTR) is much higher this year and that all the events (with the exception of a few) are all simply reporting background events that were not caused by the Covid-19 vaccines.
There’s just one tiny little problem with that explanation: there is a CDC paper that proves that they are lying. Big time.
I will show below that even if we believed everything they said, it can’t explain all the deaths and severe adverse events. The data simply doesn’t fit their hypothesis. At all.
The reality is the vaccines are extremely dangerous, they kill more than they save for every age range (it’s worse the younger you are), and they should be halted immediately, not green lighted like the FDA committee just did. All vaccine mandates should be rescinded.
The CDC paper
In a nutshell, there is a paper written by five CDC authors, The reporting sensitivity of the Vaccine Adverse Event Reporting System (VAERS) for anaphylaxis and for Guillain-Barré syndrome, that was published a year ago in the peer-reviewed scientific literature.
The paper claims that serious adverse events in the past have been under-reported by at most a factor of 8.3 (known as the under-reporting factor (URF)).
This means that in the best possible scenario, where there is full reporting (i.e., where the URF=1 and the PTR, defined as the avg URF/current URF, is 8.3), a reporting rate of serious adverse events that is 8.3X higher than the previous reporting rate for that symptom could be safely ignored as simply due to a higher propensity to report the naturally occurring rate of background events.
While theoretically you could have a URF of <1, this is unlikely since the HHS verifies all records before they are put in the database and eliminates duplicates. There are mistakes that happen but they are minor, e..g, we know of 2 gamed records out of the 1.6M VAERS reports. So the minimum URF would be 1 and it would be nearly impossible to achieve from a practical standpoint.
Here’s the problem. This year, with the COVID vaccines, there are a huge number of serious adverse events that are reported at a rate that is more than 8.3X higher than previous years. In fact, nearly every serious event I investigated was elevated from previous years by significantly more than this. I documented this in an important video on VAERS serious adverse event reports that I hope everyone will watch.
Unfortunately, none of the people at the FDA, CDC, or on their respective outside committees has ever watched that video. If they did, they would immediately realize the enormous mistakes that have been made and I’m sure take corrective action.
But cognitive dissonance prevents them from watching the video. I think the only way to force them to watch the video would be to physically strap them in a chair and put clamps on their eyes as was done in the movie “A Clockwork Orange.”
How do you explain the rates of pulmonary embolism?
The most stunning serious adverse event I found was pulmonary embolism (PE).
As I show in the video, the average annual number of reports of PE per year in VAERS for all vaccines was 1.4. So we’d expect to see at most 11.6 PE events this year according to the belief system of the FDA and CDC. Well, one tiny little problem: with the COVID vaccines, there were 1,131 reports, nearly a 100-fold increase over the “best case” scenario. Please watch the video on VAERS serious adverse event reports to see this for yourself.
Also, for those suffering from “cognitive dissonance syndrome” (this is a common affliction of people who think the vaccines are safe), the increase in reports isn’t due to increased rates of vaccination either as we explain in this paper which shows historical vaccination rates among various age groups.
In other words, even if you totally buy the bullshit argument of the FDA and CDC (which they never justified with analysis or data) that the URF=1 this year, it still means that 99% of the reports of pulmonary embolism (PE) are unexplainable. They must be caused by “something” and that something has to be very big and it has to be correlated with the administration of the vaccine because the PE reporting rate was correlated with the vaccine administration.
If these PE events weren’t caused by the vaccine, then what caused them?
Nobody can explain that. Nobody even attempts to explain it. Nobody even wants to talk about it.
But since the mainstream media and fact checkers are completely tone deaf to safety reports, they never ask the question. They never will. It would explode the whole false narrative.
We kill 15 people to maybe save 1. Are we nuts?
Furthermore, if we use the same methodology as used by the CDC in their paper to determine the actual underreporting factor for this year, but we use a much more accurate reference, we find that the best estimate for the minimum URF is 41. For less serious events you’d use a higher number since healthcare workers and consumers are far less likely to report less serious events. So using 41 is always “safe” in that it will not overestimate any event.
This means that we’ve killed well over 150,000 Americans so far, and all of those deaths had to be caused by the vaccine because there is simply no other explanation that fits all the facts. See this paper for the details. The paper also details 7 other ways that the number was validated and none of those methods used the VAERS data at all. This makes it impossible for anyone to credibly attack the analysis. Nobody wants to debate us on this.
And Pfizer’s own Phase 3 study showed that we save only 1 COVID death for every 22,000 people we vaccinate (you have to see Table S4 in the supplement to learn that 2 people died from COVID who were unvaccinated and 1 person died from COVID who got the vaccine, so a net savings of 1 life).
We have fully vaccinated almost 220M Americans which means we may save an estimated 10,000 lives from COVID per the Pfizer study which is the most definitive data we have (since “real scientists” ONLY trust the data in the double-blind randomized controlled trials).
Yet the VAERS data shows we killed over 150,000 Americans from the vaccine to achieve that goal.
In other words, we killed 15 people for every COVID life we might save.
But it’s worse than that because the Pfizer study was done pre-Delta. The Pfizer vaccine was developed for Alpha variant and is less effective against Delta. So our numbers are even more extreme.
This means of course that the FDA, CDC, and their outside committees are all incompetent in their ability to spot safety signals. They couldn’t even spot the death safety signal. It also means that the vaccine mandates are immoral and unethical.
Inconvenient truth: vaccine-induced myocarditis is neither rare or mild
When we apply the proper URF to the myocarditis data, we find that myocarditis goes from a “rare” event to a common event.
Using data from the CDC and applying the correct URF, for 16 year-old boys, the rate of myocarditis is 1 in 317 as we can see from this slide from our All you need to know deck. That’s not rare. That’s a train wreck. [MORE]
Floyd Mayweather (whose success doesn't depend upon elite whites) Stands w/Kyrie Irving Over his Vaccine Refusal while Showcase Blacks Pretend Healthy Athletes are Dangerous and Parrot Their Masters
/From [theFinalCall] Kyrie Irving and all NBA players have it better than most Americans when it comes to understanding the deadly impact of the COVID-19 “vaccine.” Every night they play before massive crowds cheering their every move. Brother Kyrie plays for the Brooklyn Nets at the 17,000-seat Barclays Center arena.
Every game, whether home or away, he can look around and see the appalling number of people killed by the COVID-19 “vaccine.” It is a gruesome sight. This is the number of people who were, for the most part, living normal lives. Then came the virus and with it the deadly vaccine and takeover of the minds of the people by the most relentless, suffocating, corporate media campaign in U.S. history.
According to the CDC’s own calculations, at least 17,128 Americans have been killed by the “jab” that Fauci and his depopulation plotters have deployed and forced into 190 million arms.
The NBA is filled with Black men in exemplary physical condition. They have reached that level of athletic proficiency by supporting their God-given talent with diligent and disciplined self-care for their overall health. They are acutely aware of the effects of the government poison. Beyond the homicides, 26,200 Americans have been permanently injured; 84,000 hospitalized; 92,000 have required urgent care after receiving the shots. That stunning number of reported deaths and injuries represents just one percent of the actual number—most deaths and injuries from the COVID killshot are unreported.

“DOLLY WANT A CRACKER?” MASTER SAID SO, MASTER SAID SO. guess what? FUCK A SNAG - $nitch-ass Negro Aiding Government. 2) COINTEL-BROs. 3) Smile Negro And Grin - while I put it in. 'SNAGs are coin-operated, sniggering negroes on the stroll who support the psychopathological dominant minority elite European global racist-supremacist mindset and Agenda along with its narcissistic projections and population control objectives (genocide and eugenics). [MORE] (pictured Above; SNAGS on ESPN perform for their masters in The Spectacle. THEY ARE all THE OPPOSITE OF SELF-MADE, UNDEFEATED BOXING LEGEND FLOYD MAYWEATHER. Fuck all pictured above IN ESPN’S SNIGGER SHOWCASE, PROMOTING BLACK MEDIOCRITY ON BEHALF OF RWS AND OBEDIENCE TO AUTHORITY)
Furthermore, FUCK A COIN OPERATED SAMBO ROLEBOT (Showcase Black) . According to FUNKTIONARY
Sambo - a self-loathing Negro lacking self-knowledge. "A willing slave gets upset if you refuse to acknowledge his or her master. Usually when people say 'act responsibly,' what they mean is: 'cowtow to the conforming lies we call truths.'" -George Battailles. The old saying still holds true: "The value of a dollar, will never, ever drop as low as the standards of some miseducated self-hating Negroes to obtain it." (See: Sniggers, Mentacide, Self-Hate & Slavery)
shenanigger - a Negro (neo-lawn-jockey) who carries out Step-n-Fetchit type activities/actions (shenanigans) for the dominant immoral majority (the psychopathic white power semi-organism), i.e., the Rhodes, Rothschild, Anglo Saxon Zionist power clique, unknowlingly at the expense of him/herself and knowlingly at the expense (sell-out/buy-out) of his people and culture. (See: McNegro, Coin-Operated, The Moteasuh Tribe, Sambo & SNigger).
Players know they are part of the notorious NBA plantation system that cares only for the profits owners can wring out of Black bodies. Commissioner Adam Silver, who has no perceptible athletic talent and no medical education at all, has determined that on his plantation “it’s perfectly appropriate that…cities have passed laws that require people who both work and visit arenas to be vaccinated. That seems to be a responsible public health decision.”
Black players have balked at taking medical advice from the profit-driven administrator, and several powerful NBA athletes have refused to become public guinea pigs for him and the team owners. The Lakers’ Kent Bazemore was clear about how he Eats to Live: “I do everything I can to strengthen my immune system, with hours upon hours of cooking, preparing my meals at home, really being conscious of what I put in my body and taking care of my health.”
He continued, “My family has a history of heart disease and all these different things, and I’m trying to turn that around for my lineage. So, I’m taking it upon myself to do everything I can to keep my immune system strong and live a healthy and long life.” Bazemore ultimately took the lethal shot but “seemed to imply that signing with the team was contingent on his agreement to be vaccinated.”
A powerful few say they will not be forced to take the injections nor bullied into disclosing their vaccination status, a stance that puts these superstars in the company of the highly educated. According to a Carnegie Mellon study of vaccine attitudes, the highest “vaccine hesitancy” was “among those with a PhD.” It is the most intelligent of players who are refusing to risk their lives to enrich Pfizer, Moderna, and Johnson & Johnson and further the Depopulation Agenda. For that they face threats of suspensions, terminations, fines, and media harassment.
Golden State Warriors star Andrew Wiggins applied to the NBA for a religious exemption from taking the 17,000-death shot and was summarily denied in a rude public statement designed by Silver to send a chill through any other players who might also seek exemptions: “The NBA has reviewed and denied Andrew Wiggins’ request for religious exemption. Wiggins will not be able to play in Warriors home games until he fulfills the city’s vaccination requirements.”
Silver added, “Unvaccinated players who do not comply with local vaccination mandates will not be paid for the games they miss.” Silver chose to scoff at Wiggins’s commitment to his religious principles, offering a vivid reminder of the righteous stand boxer Muhammad Ali against the satanic killers of his day. Wiggins adheres to what God has mandated: fighting disease through fresh air, sunlight, and nutritious foods—all of which boost immunity to a virus with a near 100% survival rate.
Wiggins also said no one in his family is vaccinated. “It’s not really something we believe in as a family. I’m 26. I have two kids. I want more kids. I’m trying to do something that will generate as much money as I can for my kids and my future kids, trying to make generational wealth.
This is a significant observation on the part of a young man in his twenties. But it is no coincidence that Andrew Wiggins is a conscious man driven by a set of spiritual principles and dietary laws. He is the son of Chicago Bulls’ Mitchell Wiggins, whose teammate Darius Muhammad brought to the Final Call Building along with other members of the Bulls back in the early 1980s to hear the Honorable Minister Louis Farrakhan.
After he succumbed to pressure and took the injection, a rueful Wiggins no doubt expressed the feelings of many fellow athletes: “I feel like the only options [were] to get vaccinated or not play in the NBA. Hopefully, it works out in the long run and in 10 years I’m still healthy….[G]etting vaccinated, that’s going to be something that stays in my mind for a long time. It’s not something I wanted to do, but kind of forced to. I guess you don’t own your body. That’s what it comes down to. If you want to work in society today, then I guess they made the rules of what goes in your body and what you do. Hopefully, there’s a lot of people out there that are stronger than me and keep fighting, stand for what they believe, and hopefully, it works out for them.”
Teammate Draymond Green addressed the pressure being applied to these multi-million-dollar athletes: “I think there is something to be said for people’s concern about something that’s being pressed so hard. Like, why are you pressing this so hard? Like, so much, just pressing and pressing and pressing. I think you have to honor people’s feelings and their own personal beliefs—and I think that’s been lost when it comes to vaccinated and non-vaccinated.
And it kinda sucks that that’s been lost, because you’re essentially not giving anyone…you say we live in the land of the free? Well you’re not giving anyone freedom because you’re making people do something, essentially. Without necessarily making them, you’re making them do something. And that goes against everything that America stands for, or ‘supposedly’ stands for.” [MORE]
Expert Asks FDA, “How many have to die before you pull the plug?” FDA Panel Recommends Pfizer Injection for Young Kids Despite Evidence Vax is Unnecessary and Risk of Injury is Greater than COVID Risk
/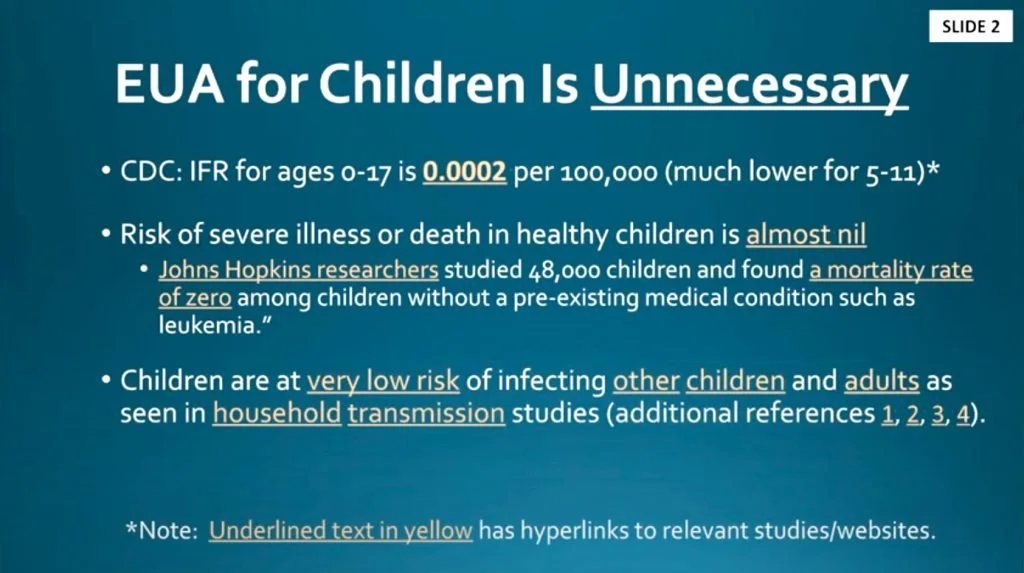
PROTECTING KIDS AGAINST WHAT? From [CHD] and [MORE] The U.S. Food and Drug Administration’s (FDA) advisory committee today endorsed Pfizer’s COVID vaccine for children ages 5 to 11, despite strong objections raised during the meeting by multiple scientists and physicians.
The vote passed with 17 supporting it and one abstention.
Before the shots can be rolled out, the FDA will have to formally authorize the vaccine, and the Centers for Disease Control and Prevention (CDC) must also weigh in with its own recommendations — but the Biden administration’s announcement last week that it has already ordered 68 million doses of the pediatric vaccine suggests Pfizer’s request will sail through.
During today’s meeting, the Vaccines and Related Biological Products Committee (VRBPAC) heard evidence from Pfizer and regulators, and listened to concerns from numerous experts.
According to the FDA website, as of Oct. 25, the agency had received 139,470 comments from the public prior to today’s meeting — a number federal officials described as strikingly high.
As he opened the meeting, Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research (CBER), said, “I want to acknowledge the fact that there are strong feelings that have clearly been expressed by members of the public both for and against” authorization.
Marks stressed the only question before the experts was whether shots should be allowed, not whether to mandate them, the New York Times reported.
The dose for younger children would be one-third the strength given to people 12 and older, with two shots given three weeks apart.
Based on CDC data presented during the meeting, among children 5 to <12 years of age, there have been approximately 1.8 million confirmed and reported COVID cases since the beginning of the pandemic, and only 143 COVID-related deaths in the U.S. through Oct. 14.
In this same age group, there were 8,622 COVID-related hospitalizations through Sept 18.
“This translates to cumulative incidence rates of approximately 6,000 and 30 per 100,000 for confirmed COVID cases and COVID-related hospitalizations, respectively, among children 5 to <12 years of age,” Pfizer’s application said.
Children with underlying medical conditions, such as asthma, diabetes and obesity, made up two-thirds of severe COVID cases.
Pfizer provided safety data on two study cohorts of children ages 5 to 11, both of roughly equal size. The first group was followed only for about two months, the second for only two-and-a-half weeks.
The two-month cohort included 2,268 children ages 5 to 11. Of the 2,268 children, 1,518 received the vaccine and 750 received a placebo. Each received two shots spaced three weeks apart.
Pfizer’s study found its vaccine was about 91% effective against symptomatic COVID in children, based on 16 cases of COVID in the placebo group and three cases in the vaccinated group over the brief follow-up period.
Most side effects occurred within a couple of days and included pain at the injection site, fatigue, headache, muscle pains and chills, Pfizer said.
According to Pfizer, the number of participants in the current clinical development program was “too small to detect any potential risks of myocarditis associated with vaccination.”
Long-term safety of Pfizer’s COVID-19 vaccine “to evaluate long-term sequelae of post-vaccination myocarditis/pericarditis” in participants 5 to <12 years of age will not be studied until after the vaccine is authorized for children,” Pfizer’s application noted.

Pfizer data insufficient, kids’ risk of vaccine injury greater than COVID risk, experts say
Experts raised concerns over the lack of safety and efficacy data presented by Pfizer for use of its COVID vaccine in younger children, and they pointed to increasing safety signals based on reports to the Vaccine Adverse Event Reporting System (VAERS).
They also questioned the need to vaccinate children — whose risk of dying from COVID is “almost nil” — at all.
According to Dr. Meryl Nass, member of the Children’s Health Defense Scientific Advisory Panel, Pfizer once again did not use all of the children who participated in the trial in their safety study.
“Three thousand children received Pfizer’s COVID vaccine, but only 750 children were selectively included in the company’s safety analysis,” Nass said. “Studies in the 5-11 age group are essentially the same as the 12-15 group — in other words, equally brief and unsatisfying, with inadequate safety data and efficacy data, with no strong support for why this type of immuno-bridging analysis is sufficient.”
Nass said, “All serious adverse events were considered unrelated to the vaccine.”
During the meeting and in its FDA application, Pfizer argued children should be vaccinated to prevent SARS-CoV-2 transmission, yet the company did not assess asymptomatic transmission.
Dr. Ofer Levy, a VRBPAC member, asked for evidence that Pfizer’s vaccine prevents transmission.
Dr. William Gruber, senior vice president of Pfizer Vaccine Clinical Research and Development, said they did not assess whether the vaccine prevents transmission, but said there is evidence the vaccine prevents transmission in adults.
When questioned further, Gruber was unable to cite specific evidence to back his assertion.
Steve Kirsch, founder of the COVID-19 Early Treatment Fund, asked the panel how they could do a risk-benefit analysis with Pfizer’s COVID vaccine if they did not know the CDC’s VAERS under-reporting factor (URF).
Kirsch asked:
“How can you do a risk-benefit of analysis of COVID vaccines if you don’t know the URF? This is extremely, extremely important. You have been assuming it has been one. It is not one. Using a URF of 41, which is calculated using CDC methodology, we find over 300,000 excess deaths in VAERS. If the vaccine didn’t kill these people, what did?”
“How many Americans have to die before you pull the plug?” Kirsch asked.
Kirsch also questioned the panel on why Maddie de Garay’s severe adverse reaction to the Pfizer vaccine, which left her paralyzed, was not reported by the company to the FDA.
Dr. Jessica Rose, viral immunologist and biologist, told the panel EUA of biological agents requires the existence of an emergency and the nonexistence of alternate treatment.
“There is no emergency and COVID-19 is exceedingly treatable,” Rose said.
In a peer-reviewed study co-authored by Rose, myocarditis rates were significantly higher in people 13 to 23 years old within eight weeks of the COVID vaccine rollout.
In 12- to15-year-olds, Rose said, reported cases of myocarditis were 19 times higher than background rates.
“In an act of censorship, this paper has been temporarily removed and it has now been killed without criticism of the work,” Rose said, noting the timing of the removal was strange.
Rose said tens of thousands of reports have been submitted to VAERS for children ages 0 to 18.
Rose explained:
“In this age group, 60 children have died — 23 of them were less than 2 years old. It is disturbing to note that “product administered to patient of inappropriate age was filed 5,510 times in this age group. Two children were inappropriately injected, presumably by a trained medical professional, and subsequently died.”
Dr. Josh Guetzkow, a senior lecturer at the Hebrew University of Jerusalem, said expanding the EUA to children is unnecessary, premature and will do more harm than good.
Guetzkow said there is no emergency for children, especially healthy ones whose risk of severe illness and death is “almost nil.”
Guetzkow said kids with pre-existing conditions and prior COVID infections were not included in Pfizer’s study, so including them in the EUA is negligence.
“Pfizer’s trial is woefully underpowered to detect specific safety concerns, such as myocarditis, just like the adolescent study was, and if they weren’t able to detect an unexpected safety concern there, they wouldn’t be able to here,” Guetzkow said.
Guetzkow said:
“In Pfizer’s study, only .5% of controls were dropped due to important protocol violations, versus 3% in the treatment group. The odds of that happening by chance are 1 in 10,000. This deviation is poorly explained with no ITT analysis. The study is not double-blind and may be subject to bias. Most VSD safety monitoring programs have not reported results, why not wait?”
Guetzkow said, “from CDC reports, we can expect that for every 18 child hospitalizations prevented, at least 43 will end up in the hospital for all causes following vaccination,” yet, the “FDA’s risk-benefit analysis only counts myocarditis hospitalization.”
“Why ignore the V-safe data, and shouldn’t FDA verify Pfizer’s efficacy and immunobridging analysis first?” he asked.
Guetzkow said VAERS shows alarming safety signals, which cannot be attributed to increased vaccination, simulated reporting or COVID infections.
“We calculated the ratio of adverse events reported per million Pfizer vaccinations to reports per million flu vaccinations among teenagers to see what to expect in children. Serious events are reported 51% more often for Pfizer, deaths 47 times, life-threatening conditions 49 times,” Guetzkow said.
Guetzkow asked the panel to look at the data on COVID vaccines compared to flu vaccines. Pointing to the data on reproductive organs, Guetzkow asked, “why would we expect children to take these risks to protect adults?”
There are more than 900 types of adverse events reported after Pfizer vaccination that have never been reported after flu vaccines, including 11 cases of multisystem-inflammatory syndrome (MS-C) that occurred without previous history of COVID infection, Guetzkow said.
He added that if the panel was considering authorizing Pfizer’s COVID vaccine to prevent MS-C — as Pfizer’s application suggested as one of the reasons they should — the panel should reconsider.
During another part of the meeting, Julia Barnes-Weise, director of the Global Healthcare Innovation Alliance Accelerator, said pharmaceutical companies have concerns.
“One of them is, especially for a not-yet-approved vaccine, that they could be held liable for any injury that that vaccine seems to have caused,” Barnes-Weise said.
In a preliminary analysis last week, FDA reviewers said protection would “clearly outweigh” the risk of a very rare side effect in almost all scenarios of the pandemic, PBS News Hour reported.
Children’s Health Defense (CHD) said yesterday it would take legal action against the FDA if it granted EUA for the Pfizer-BioNTech vaccine for children 5- to 11- years old.
Robert Kennedy's Organization CHD Threatens to Sue Government for Recklessly Endangering Children if FDA Authorizes Pfizer “Vaccine" for Kids 5 to 11 Years Old
/
From [HERE] Children’s Health Defense (CHD) today said it will take legal action against the U.S. Food and Drug Administration (FDA) if the agency grants Emergency Use Authorization (EUA) for the Pfizer-BioNTech SARS-CoV-2 vaccine for children aged 5-11.
In a letter signed by Robert F. Kennedy, Jr., CHD chairman and chief legal counsel, and Dr. Meryl Nass, member of the CHD Scientific Advisory Committee, Kennedy and Nass wrote:
“CHD will seek to hold you accountable for recklessly endangering this population with a product that has little efficacy but which may put them, without warning, at risk of many adverse health consequences, including heart damage, stroke, and other thrombotic events and reproductive harms.”
The letter was addressed to Dr. Arnold Monto, chairman of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC), committee members and all FDA staff.
VRBPAC members are set to meet Tuesday to consider and likely vote on whether to grant EUA for the Pfizer vaccine for 5- to 11-year olds.
In May, the FDA authorized Pfizer’s vaccine for 12- to 15-year-olds. Moderna and Johnson & Johnson vaccines have not yet been authorized for children under 18.
The letter outlines 12 reasons the FDA should not authorize the pediatric vaccine and provides supporting evidence to back up each argument.
Read the letter:
Dear Chairman Monto, VRBPAC Members and FDA Staff:
We write to you on behalf of Children’s Health Defense (CHD), a non-profit organization devoted to the health of people and the planet. We have actively followed your work to evaluate, authorize and approve vaccines for the American public and particularly children.
We are aware that you are likely to authorize Pfizer’s BioNTech SARS-CoV-2 vaccine for children aged 5-11 at your meeting on Oct. 26. Your authorization thus will expose over 20 million children in the U.S., and millions more around the world, to potential COVID-19 vaccination of an Emergency Use Authorization (EUA) product.
We are writing to put you on notice that should you grant EUA status to this pediatric EUA vaccine, CHD is poised to take legal action against you and other Vaccines and Related Biological Products Advisory Committee (VRBPAC) voting members as well as the FDA.
CHD will seek to hold you accountable for recklessly endangering this population with a product that has little efficacy but which may put them, without warning, at risk of many adverse health consequences, including heart damage, stroke and other thrombotic events and reproductive harms.
We briefly outline why such authorization would be reckless:
1. The risks demonstrably outweigh the benefits of COVID vaccination for young children.Deaths and hospitalizations are rare and have been inflated inaccurately.
2. Nearly half of all children have natural immunity to COVID, according to the Centers for Disease Control and Prevention (CDC). There is no ethical justification for superfluous vaccination that will put children at elevated risk of vaccine harm.
3. Some children likely will die or be permanently injured from these vaccines based on the authorization for children 12-16.
4. The clinical trials for the pediatric vaccine were too small to detect safety signals for a population in the millions.
5. There are no long-term safety data for COVID vaccination of young children, making this an experiment rather than appropriate medical prevention.
6. Unethical coercive pressure will be applied to children and their parents, as has occurred with older children and adults. To grant authorization is to abet this unethical coercion that violates the Nuremberg Code’s first principle.
7. There is no available care for children injured by COVID shots. The science and medicine have not yet developed, and most families will be unable to cover the costs of potential catastrophic injuries.
8. VRBPAC members should not participate in an exercise disguising a foregone conclusion.The president’s purchase of 65 million pediatric doses, the CDC guidance for COVID vaccine delivery, the American Academy of Pediatrics’s promotion of COVID vaccination for children all call into question whether this committee’s deliberations mean anything.
If the administration is unprepared to wait for your advice, let alone heed it, you should signify your disapproval on behalf of the country the FDA is meant to protect.
9. First, do no harm. You are physicians who owe a duty to patients and medical ethics. If you authorize these shots, given all you know, will you be upholding your oath? If not, is it possible that your acts could later be seen as reason to remove your medical licenses?
10. The liability-free nature of your deliberations may not stand the test of time. In the fullness of time, your decisions may not have the liability protection that they currently enjoy. Under the PREP Act of 2005, all actors advancing an EUA agenda for medical countermeasures enjoy liability protection, absent willful misconduct.
Nonetheless, if at a later point these shots are deemed non-therapeutic gene products that you knowingly and recklessly authorized, and which were then distributed to children as a direct result of your decision, it is possible that liability could later attach.
11. There is no COVID emergency for children of this age.
12. There are safer drugs that could be used prophylactically and therapeutically for COVID in children. There is extensive and compelling medical evidence for this assertion — and the choice to eschew use of these drugs in favor of a demonstrably dangerous vaccine is arbitrary and capricious.
We ask that you carefully consider all the information above before making any recommendation to authorize Pfizer’s vaccine in the 5 through 11 year age group at your meeting on Tuesday, Oct. 26.
Sincerely yours,
Let’s investigate the basis for claims that children aged 5 through 11 need to be vaccinated for COVID.
1. The truth is that children aged 5-11 are at extremely low risk of hospitalization, death, MIS-C or Long COVID.
a. What is the actual risk of hospitalization, death and MIS-C in aged 5 through 11-year-old children? This age group has the lowest rate of severe disease and death than all other age cohorts.
CDC reports 94 COVID-19 deaths with COVID since Jan. 1, 2020, in the 5 through 11 age group. However, CDC designates these as deaths “involving COVID” or “with COVID” rather than due to COVID, according to CDC’s chart below.
b. In the October 2021 Pediatrics, a report by David McCormick et al. showed that of 112 pediatric deaths associated with SARS-CoV-2, 86% had comorbidities, especially obesity, neurologic and developmental conditions. The mean age of decedents was 17.
c. It is impossible to separate deaths with COVID from those due to COVID in the U.S. because the CDC does not distinguish them. But what we do know is that child deaths due to COVID in Germany, according to the BILD newspaper, were 20 in May 2021, in a country with 85 million people.
Pediatric deaths were “under 30” through March 2021, according to the UK government, with 60 million people. [MORE]
Dr. Sucharit Bhakdi: 'COVID Vaccines are Killing People Not Protecting Them. Governments, Dependent Media and Pharmaceutical Companies are Complicit in Genocide and Crimes Against Humanity'
/Dr. Sucharit Bhakdi is a Thai-German microbiologist who has been speaking out against the COVID-19 hysteria since the beginning of the crisis. He was a post-doctoral researcher at the Max Planck Institute of Immunobiology and Epigenetics in Freiburg and at The Protein Laboratory in Copenhagen. Dr. Bhakdi joined the Institute of Medical Microbiology at Giessen University and named chair of Medical Microbiology at the University of Mainz. Dr. Bhakdi has published over three hundred articles in the fields of immunology, bacteriology, virology, and parasitology, for which he has received numerous awards and the Order of Merit of Rhineland-Palatinate. [MORE]
YOU ARE BEING LIED TO BY GOVERNMENTS, CORPORATIONS AND THEIR MEDIA AND YOU ARE BEING EXPERIMENTED ON [but enjoy your illusions]. From [EvidenceNotFear] COVID-19 is a disease defined by symptoms and not a virus. It’s therefore not transmitted nor can you test for it using nasal or throat testing kits. SARS-CoV-2 is the coronavirus that prompted the worldwide pandemic response.
In at least 80% of cases, the virus produces either no symptoms or a mild cold-like illness. For most of the population, the infection fatality rate for COVID-19 is 0.15%-0.2%. This brings it close to seasonal flu which is around 0.1%-0.2%.
Children have a greater chance of being struck by lightning than dying of COVID-19.
Adults are more likely to die in a car accident.
The vast majority of us have no risk of dying from COVID-19. Studies show that 99.94% survive COVID-19 and will be resistant for a long time. The QCovid risk calculator from Oxford University can be used to calculate your risk of death or hospitalisation.
The people at risk from COVID-19 are clearly defined and should be protected with targeted measures. Children are not susceptible to it nor do they transmit the virus.
However, COVID-19 can be deadly for older and vulnerable people so it’s important to protect them. This will help eliminate hospital overcrowding. Nevertheless, the average age of someone who dies from COVID-19 is around 82 years. This is higher than the average life expectancy in the UK which is around 81 years.
Lockdowns will prevent population immunity and prolong the problem. Isolating the vulnerable and allowing the remaining population to practice safe distancing has been a historically proven way of dealing with flu-like viruses.
Fear instilled by panic and hysteria in the media is causing more people to die. Many are refusing to seek medical care because they are afraid to leave their homes. Others have not received proper medical care because of new procedures put in place.
There is no strong medical evidence that face masks prevent infection with respiratory viruses, including COVID-19. This is even stated in government guidelines for businesses.
COVID-19 style social distancing has little to do with the historically proven practice of isolating sick people. There is no scientific evidence that these measures prevent the spread of the disease.