A Pfizer Worker Blows the Whistle on Vax Data Cover-Up but Dependent Media Can't Hear. Pfizer Hid Info that the Vax Caused Severe, Long-term, Unresolved injuries. FDA Now Wants 75 yrs to Release Data
/
According to Brook Jackson, a whistleblower who worked on Pfizer’s Phase 3 COVID jab trial, data were falsified, patients were unblinded, the company hired poorly trained people to administer the injections, and follow-up on reported side effects lagged way behind
The FDA did not follow up on Jackson’s complaint or investigate the allegations before granting full licensing to Pfizer’s Comirnaty shot
FDA now wants 75 years to drip out the data it relied on to grant full licensing to Comirnaty
An adverse event report from Pfizer, covering December 2020 through the end of February 2021, shows the shot causes severe and often long-term, unresolved injuries
Pfizer’s data also show the shot causes severe injuries in pregnant and nursing women. Based on these data alone, which the FDA was aware of at the end of April 2021, the Pfizer shot should have been pulled from the market
From [MERCOLA] According to Brook Jackson, a whistleblower who worked on Pfizer’s Phase 3 COVID jab trial in the fall of 2020, data were falsified, patients were unblinded, the company hired poorly trained people to administer the injections, and follow-up on reported side effects was significantly delayed.
Her testimony was published November 2, 2021, in The British Medical Journal by investigative journalist Paul Thacker, who noted that:1
“[F]or researchers who were testing Pfizer’s vaccine at several sites in Texas during that autumn, speed may have come at the cost of data integrity and patient safety … Staff who conducted quality control checks were overwhelmed by the volume of problems they were finding.”
December 2, 2021, The Last American Vagabond interviewed Jackson (video above2) about what she saw while working on Pfizer’s trial. Jackson is a trained clinical trial auditor with more than 15 years’ experience in clinical research coordination and management.
She had previously held a director of operations position before she was hired in early September 2020 by the Ventavia Research Group, a research organization charged with testing Pfizer’s COVID jab at several sites in Texas. Right from the start, Jackson was struck by the chaotic nature of the operation.
She also felt the informed consent was inadequate, considering the novel nature of the mRNA gene transfer technology. On top of that, she found the crash cart contained expired medications, and some important emergency medications — were a participant to suffer an acute adverse event — were missing entirely.
Data Forgery Among the Many Problems Identified
Jackson claims she repeatedly informed her superiors of poor laboratory management, patient safety concerns and data integrity issues. When she realized her concerns were ignored, she finally filed a complaint with the U.S. Food and Drug Administration. In her complaint to the FDA, Jackson listed a dozen incidents of concern, including the following:
Participants were not monitored by clinical staff after receiving the shot
Patients who experienced adverse effects were not promptly evaluated and protocol deviations were not being reported
The Pfizer injection vials were stored at improper temperatures
Laboratory specimens were mislabeled
Later that same day, Jackson was fired. According to her separation letter, management decided she was “not a good fit” for the company. According to Jackson, this was the first time she’d ever been fired in her 20-year career as a clinical research coordinator. As noted by Thacker:3
“In a recording of a meeting in late September 2020 between Jackson and two directors a Ventavia executive can be heard explaining that the company wasn’t able to quantify the types and number of errors they were finding when examining the trial paperwork for quality control. ‘In my mind, it’s something new every day,’ a Ventavia executive says. ‘We know that it’s significant.’
Ventavia was not keeping up with data entry queries, shows an email sent by ICON, the contract research organization with which Pfizer partnered on the trial. ICON reminded Ventavia in a September 2020 email: ‘The expectation for this study is that all queries are addressed within 24hrs.’
ICON then highlighted over 100 outstanding queries older than three days in yellow. Examples included two individuals for which ‘Subject has reported with Severe symptoms/reactions … Per protocol, subjects experiencing Grade 3 local reactions should be contacted. Please confirm if an UNPLANNED CONTACT was made and update the corresponding form as appropriate.’
According to the trial protocol a telephone contact should have occurred ‘to ascertain further details and determine whether a site visit is clinically indicated.’ Documents show that problems had been going on for weeks.
In a list of ‘action items’ circulated among Ventavia leaders in early August 2020, shortly after the trial began and before Jackson’s hiring, a Ventavia executive identified three site staff members with whom to ‘Go over e-diary issue/falsifying data, etc.’ One of them was ‘verbally counseled for changing data and not noting late entry,’ a note indicates.”
Jackson’s disclosures were recently featured in the Italian documentary, “Pfizergate.”4,5 The documentation she gathered are available for download on the COVID Vaccine Reaction’s website.6
Ventavia, Pfizer and FDA Ignore Accusations
Strangely enough, the extent of Ventavia’s effort to defend itself has been to deny that Jackson ever worked on the Pfizer trial — a charge that is verifiably false, as she has documentation proving she was assigned to work on the trial.7
Pfizer has also remained mum on the issue. The company did not reply to any of The BMJ’s questions, one of which was whether Ventavia’s data were incorporated into Pfizer’s safety and efficacy analyses.
We do know, however, that none of the problems Jackson raised in her complaint to the FDA were noted or addressed in Pfizer’s briefing document, submitted to the FDA’s advisory committee meeting December 20, 2020, when its emergency use authorization application was reviewed.
The FDA went ahead and gave the Pfizer jab emergency use authorization the very next day, despite being in receipt of Jackson’s complaint, which ought to have put the brakes on the FDA’s authorization. At bare minimum, they should have investigated the matter before proceeding.
The BMJ has tried to get answers from the FDA as to why it has not inspected any of Ventavia’s trial sites in the wake of Jackson’s accusations, and whether other complaints about the trial have been received. An FDA spokesperson told The BMJ the agency cannot comment as it is “an ongoing matter,” whatever that means.
The FDA did say, though, that it has “full confidence in the data that were used to support the Pfizer-BioNTech COVID-19 Vaccine authorization and the Comirnaty approval.” Considering they’ve not investigated Jackson’s complaints, their vote of confidence doesn’t strike me as particularly convincing.
Other Ventavia Witnesses Speak Out
Jackson wasn’t the only employee to get sacked from Ventavia after raising concerns about the integrity of the Pfizer trial. According to Thacker, several other Ventavia employees either left or were fired. Among them is a Ventavia official who had participated in the late September meeting cited above. Thacker writes:8
“In a text message sent [to Jackson] in June the former official apologized, saying that ‘everything that you complained about was spot on.’ Two former Ventavia employees spoke to The BMJ anonymously for fear of reprisal and loss of job prospects in the tightly knit research community. Both confirmed broad aspects of Jackson’s complaint.
One said that she had worked on over four dozen clinical trials in her career, including many large trials, but had never experienced such a ‘helter skelter’ work environment as with Ventavia on Pfizer’s trial.
‘I’ve never had to do what they were asking me to do, ever,’ she told The BMJ. ‘It just seemed like something a little different from normal — the things that were allowed and expected.’”
According to these whistleblowers, problems persisted after Jackson’s firing. One of them claims there were, on several occasions, not enough staff to test trial participants who reported COVID-like symptoms.
Laboratory confirmed symptomatic COVID-19 was the primary endpoint of the trial, so this was a crucial task. An FDA review memorandum from August 2021 states that 477 trial participants with suspected COVID-19 were not tested for infection. “I don’t think it was good clean data,” the former Ventavia employee told Thacker. “It’s a crazy mess.”
Such statements clearly fly in the face of statements made by world leaders, health authorities and the mainstream media. Most, like federal health minister for Australia, Greg Hunt, have claimed the COVID shots have undergone “rigorous, independent testing” to ensure they’re “safe, effective and manufactured to a high standard.”9
Nothing we know so far supports such a conclusion. The testing has been far from rigorous and has not been independently verified.
Vaccine Adverse Events Reporting System (VAERS) data show they’re shockingly far from safe; real-world data show effectiveness wanes within a handful of months while leaving you more susceptible to SARS-CoV-2 variants and other infections; and manufacturing standards have also been shown lacking, as a variety of foreign contaminants have been found in the vials.10
Science Depends on Rigorous Data Collection
The video above is a short extract from a November 2, 2021, meeting organized by Sen. Ron Johnson, during which Peter Doshi, Ph.D., associate editor of The BMJ, reviewed some of the many concerns experts have about the integrity of the COVID jab data.
He pointed out that Pfizer’s raw trial data will not be made available until May 2025. So far, Pfizer has refused to release any of its raw data to independent investigators and, without that, there’s no possible way to confirm that what Pfizer is claiming is actually true and correct.
In other words, we’re expected to simply take the word of a company that has earned a top spot on the list of white collar criminals; a company that in 2009 was fined a record-breaking $2.3 billion in fines for fraudulent marketing and health care fraud.11 Press releases are not science. They’re marketing. Without the raw data, we have no science upon which to base our decisions about the COVID kill shot.
Doshi stressed how utterly unscientific a process we’re now following. He also points out that doctors have an ethical duty to not recommend a treatment for which they have no data. Quoting from a 2020 article he co-wrote:12
“Data transparency is not a ‘nice to have.’ Claims made without access to the data — whether appearing in peer reviewed publications or in preprints without peer review — are not scientific claims.
Products can be marketed without access to the data, but doctors and professional societies should publicly state that, without complete data transparency, they will refuse to endorse COVID-19 products as being based on science.”
“The point I am trying to make is very simple,” Doshi said. “The data from COVID vaccines are not available and won’t be available for years. Yet, we are not just ‘asking’ but ‘mandating’ millions of people to take these vaccines … Without data, it’s not science.”
FDA Wants 75 Years to Release Pfizer Trial Data
In September 2021, a group called Public Health and Medical Professionals for Transparency (PHMPT) filed a Freedom of Information Act (FOIA) request with the FDA to obtain the documentation used to approve Comirnaty, including safety and effectiveness data, adverse reaction reports and lists of active and inactive ingredients.
In their FOIA application, the PHMPT asked the agency to expedite release of the documents — a reasonable request, considering we have no raw data and the shots are being pushed on children as young as 5. When, after a month, the FDA still had not responded to the FOIA request, the PHMPT sued.13
The FDA initially asked the judge to allow them to delay the full release of all documents — a total of 329,000 pages — until 2076, doling out just 500 pages per month. The judge agreed.
A short while later, the FDA claimed it found another 59,000 pages, which would necessitate tacking on another 20 years.14 The full release, according to the FDA, can’t be completed until 2096, at which time most of us will be dead and buried. As noted by Aaron Siri, the lawyer working on the case on behalf of the PHMPT:15
"If you find what you are reading difficult to believe — that is because it is dystopian for the government to give Pfizer billions, mandate Americans to take its product, prohibit Americans from suing for harms, but yet refuse to let Americans see the data underlying its licensure."
All of that said, the initial release of some 92 pages are so damning, we won’t need hundreds of thousands of pages to make an assessment as to the safety of these shots. In fact, the data are so incredibly bad, it raises serious questions about how the FDA could possibly conclude that the Pfizer shot is safe enough to use, especially on pregnant women and children.
Shocking Revelations in First Batch of FOIA Docs
In mid-November 2021, two months after the lawsuit against it was filed, the FDA released the first batch of 91 pages,16,17 which reveal the FDA has been aware of shocking safety issues since April 30, 2021.
Cumulatively, through February 28, 2021, Pfizer received 42,086 adverse event reports, including 1,223 deaths, primarily from the U.S., U.K., Italy, Germany, France and Portugal. Of those adverse events, 25,379 were medically confirmed. Below is a chart from one of the documents,18 showing a general overview of the reported outcomes.
To have 1,223 fatalities and 42,086 reports of injury in the first three months is a significant safety signal, especially when you consider that the 1976 swine flu vaccine was pulled after only 25 deaths.
In the video above, Melanie Risdon with the Western Standard interviews Dr. Daniel Nagase, a doctor in Alberta, Canada, who was stripped of his Alberta medical license after successfully treating COVID-19 patients with ivermectin. Nagase reviews other equally devastating data in these documents.
He points out that of the 42,086 patients who were injured at some point during those first three months, 520 of them were diagnosed with a long-term disability or condition as a result. Not recovered at the time of the report were 11,361. That means 27% of those injured had not recovered from their adverse event.
When people get injured by this shot, they’re often injured very badly. Nearly 1 in 3 people who got the shot and suffered an adverse effect ended up dead, permanently disabled or with long-term, unresolved injury.
When you add it all together: the 1,223 deaths, the 520 long-term disabilities and the 11,361 who had not recovered from their injury, you end up with just over 31%.
In other words, nearly 1 in 3 people who got the shot and suffered an adverse effect ended up dead, permanently disabled or with long-term unresolved injury. “This should be front-page news,” Nagase says. How can the FDA look at this and conclude that the shot is safe? Clearly, when people get injured by this shot, they’re often injured very badly.
Pfizer Data Prove Shot Is Unsafe for Pregnant Women
On page 12 of the “Cumulative Analysis of Post-Authorization Adverse Event Reports Received Through 28-Feb-2021” document,19 you find data on pregnant and lactating women. Here too, the results are hair-raising and should have triggered a complete stop to the injection campaign of pregnant and nursing women.
Disturbingly, they did not collect comprehensive data on these women, such as which trimester they were in when they received the shots. This again points to serious problems with Pfizer’s trial data collection. How do you include pregnant women in a trial and don’t collect basic information such as how many weeks pregnant they are?
On page 12 we find that out of 124 adverse event cases involving a pregnant woman, only 49 were non-serious and 75 were serious. So, out of the 274 pregnant mothers who reported an adverse event, 27% suffered a SERIOUS adverse event, such as a miscarriage or stillbirth. “That’s an incredible danger!” Nagase says and, again, the FDA has been aware of this danger since April 30, 2021.
The data also show there’s danger for breastfeeding mothers. Of the 133 nursing mothers who filed a report, 17 of the breastfed babies — 13% — suffered an adverse event through this secondary exposure (breastmilk), a finding that Nagase calls “absolutely stupendous.”
“So, this idea that the ‘vaccine’ sheds and transfers through breastmilk is absolutely true,”he says. “It’s proven by Pfizer’s own adverse event data.”
Children at Risk for Serious Long-Term Injury
Pfizer also received 34 adverse event reports involving children under the age of 12, the youngest being 2 months old. Of those, 24 were categorized as “serious” and only 10 were “non-serious.” So, of the children who were injured, 70.6% suffered SERIOUS injury.
How can our health agencies approve this COVID shot for children under the age of 12 when a vast majority of injuries, when they occur, are serious ones? What’s more, 13 of the children who were seriously injured remained unresolved as of February 28, 2021.
According to Nagase, based on these documents alone, Pfizer’s COVID shot should have been permanently pulled from the market. The reason it wasn’t, he believes, is because the medical and regulatory systems have both been corrupted and usurped by the drug industry. They want to make money off these shots, and our health authorities are covering up proven harms in order to facilitate profitmaking.
At the end of the day, only you can decide what’s in your best interest. But please, do review the actual science before you make your decision and don’t blindly trust corporate press releases and unsupported statements of safety.
Pfizer’s own data prove it’s not safe by any reasonable definition of the word, and that’s on top of the testimony of Jackson and others who have seen just how shoddy the data gathering is.
Sources and References
A NY Times Editor Killed by Vax 1 Day after Booster Injection. Reported by a NYT Writer on a Blog. The NYT Doesn’t Report Vax Deaths, Even of Its Own Employees, to Avoid Conflict w/Vested Interests
/
On his blog Unreported Truths, NYT Times writer Alex Bereson wrote Carlos Tejada was married and had two children; he spent his career at the Wall Street Journal before joining the Times in 2016.
In July, he received a Johnson & Johnson DNA/AAV Covid vaccine. He was thankful to get it, per his Instagram page.
On Dec. 16, in Seoul, South Korea, he received a Moderna mRNA/LNP “booster.” No clinical trials have ever been conducted to examine the safety or efficacy of mixing various types of these vaccines, and Carlos did not give informed consent, as the consent form was in Korean, a language he could not read. He joked that Omicron should “hit me with your wet snot.”
If this does not wake the Times nothing will.
Black Man Exonerated and Released from Death Row 23 Years After Wrongful Conviction for Murder of White Woman. Prosecution Withheld Records/Physical Evidence that Another Man Committed the Crime
/
From [DPIC] Devonia Inman, sentenced to life in a capital murder trial in which Georgia prosecutors hid exculpatory evidence, has been exonerated 23 years after his wrongful conviction.
On December 20, 2021, one month after Judge Kristina Cook Graham granted Inman a new trial based on evidence that the prosecution had unconstitutionally suppressed multiple police records and physical evidence that another man had committed the killing, the Alapaha Judicial Circuit District Attorney Chase L. Studstill moved to dismiss all charges against Inman. Alapaha Circuit Superior Court Chief Judge Clayton Tomlinson granted the motion, exonerating Inman and ordering his immediate release.
He was convicted of murdering Donna Brown, a white woman.
Inman spoke to reporters outside the Augusta State Medical Prison following his release. “I’m happy,” he said. “It’s been a long time.”
“For 23 years, I’ve felt like my life was on hold,” his mother, Dinah Ray said. “I can breathe now.”
“At least 186 people who were wrongly convicted and sentenced to death in the United States have been exonerated since 1973. But those numbers are just the tip of the iceberg of the wrongful use of the death penalty in this country,” Death Penalty Information Center executive director Robert Dunham said. “Devonia Inman is one of more than 70 people to be exonerated in just the last five years in wrongful murder prosecutions in which district attorneys had sought the death penalty or cases in which police or prosecutors had threatened defendants or witnesses with the death penalty to coerce their cooperation in wrongful prosecutions.”
Liars @ NYT say "Covid vaccines rarely lead to problems in children.” Yet CDC Data Shows that at Least 30 Children Were Killed by COVID Injections, While Not a Single Healthy Child Has Died from COVID
/
FUCK THE MEDIA. Yesterday the NYT Times reported “The Centers for Disease Control and Prevention released two studies on Thursday that underscored the importance of vaccinating children against the coronavirus.
One study found that serious problems among children 5 to 11 who had received the Pfizer-BioNTech vaccine were extremely rare. The other, which looked at hundreds of pediatric hospitalizations in six cities last summer, found that nearly all of the children who became seriously ill had not been fully vaccinated.” [MORE]
Outside the Spectacle, that is, in reality, here on planet Earth, the FDA authorized the Pfizer vaccine for 5 to 11 year old children without sufficient safety information. It Ignored serious injuries to children in their clinical trials. Moreover, the emergency use authorization is unlawful because there is no COVID emergency for children. Also Pfizer has been granted complete immunity for any injuries or death to these children.
Many scientists and health experts have warned that vaccinating children against COVID-19 is unnecessary and extremely risky. Since the beginning of the pandemic, it has been obvious that children were at exceptionally low risk for hospitalization and death from the infection.1 Despite this, massive efforts are underway to ensure that every child gets a shot.
There is mounting evidence that the costs of inoculating children against covid-19 far outweigh the benefits. Children are at extremely low risk from COVID-19, with not a single death of a previously healthy child. [MORE]

Four Vietnamese children die in a Week After Pfizer vaccine
Vietnam on Nov. 30 rolled out its COVID vaccination program for children 15 to 17 years old with Pfizer’s vaccine. Since then, four children have died after receiving their first dose. The cause of death was “overreaction to the vaccine.” [MORE] and [MORE].
Vietnam is in the process of vaccinating nine million children aged 12-17. The vaccine in use is produced by Pfizer. As of December 6, 5.3 million doses have been administered to this age group, of which over 936,200 children have received two doses. [MORE]
Earlier this month, 16,000 physicians and medical scientists around the world signed a declaration publicly declaring that healthy children should NOT be vaccinated for COVID-19. Leading experts on flawed U.S. COVID policy issued an urgent warning at a summit last month: Young children will be harmed in an ill-advised rush to vaccinate a population with very little chance of severe infection from the virus. Apparently the media only listen and parrot the biostitutes who work for Big Pharma or the CDC.
“The real risk for healthy kids is about zero — it does appear to be lower than the flu,” said Dr. Robert Malone, inventor of the mRNA technology on which the vaccine is based. Inoculating 28 million children 5 to 11 years old, Malone told attendees of the Florida Summit on Covid, could lead to “a thousand or more excess deaths.”
“That’s a thousand kids,” he told the audience of 800 doctors, nurses and advocates. “It’s a thousand kids too many.”
In addition to other pressing COVID issues, the summit addressed three central questions about childhood vaccination. Do young children need vaccination against COVID? Are the vaccinations safe? Are unvaccinated children a threat to adults? On each, they found the government’s near-universal vaccination policy wanton and unsupported.
“Children don’t get severely ill. Children don’t die from this infection,” said Dr. Paul Alexander, a clinical epidemiologist and former senior advisor on pandemic policy in U.S. Department of Health and Human Services. “We’ve been fed a lot of misleading information.”
Though harshly criticized for keeping schools open, “Sweden had not a single death of a child from COVID,” said Dr. Richard Urso, a Texas ophthalmologist citing published data.
With the risk of serious illness low, panelists said the potential toll of vaccinating was unacceptably high, pointing to thousands of officially downplayed but real side effects and deaths. The risks to children include – but aren’t limited to – serious inflammation of the heart called myocarditis, which has been reported at three to six times the expected rate in vaccinated adolescents. A CDC study reported 14 vaccine-related deaths and 849 serious reactions in children 12 to 17 years old.
“There will be children lost with the vax — far more than ever happened with COVID,” said Dr. Peter McCullough, a widely published cardiologist and leading voice on a rational pandemic response. Doctors are guilty of “willful blindness” to vaccine hazards, he said, having “bought into this…dream that this vax if both safe and effective. It is shattering their dreams that it is not sufficiently safe.”
As of 12/24/21 the Centers for Disease Control and Prevention data shows a total of 965,843 reports of adverse events following COVID vaccines were submitted between Dec. 14, 2020, and Dec. 10, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 20,244 reports of deaths — an increase of 358 over the previous week — and 155,506 reports of serious injuries, including deaths, during the same time period — up 4,560 compared with the previous week.
Excluding “foreign reports” to VAERS, 691,884 adverse events, including 9,295 deaths and 59,767 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Dec. 10, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 9,295 U.S. deaths reported as of Dec. 10, 21% occurred within 24 hours of vaccination, 26% occurred within 48 hours of vaccination and 61% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 480 million COVID vaccine doses had been administered as of Dec. 10. This includes 279 million doses of Pfizer, 184 million doses of Moderna and 17 million doses of Johnson & Johnson (J&J).
In contrast to the NYT article, CDC data shows the VAX killed at least 48 children (age 5-17) since 12/14/2020. Do the elites at the NYT think CDC’s own data is fake? Instead of parroting whatever Big Pharma tells them the “reporters” could actually find an interview the parents of the child who died from the Vax on 11/22/21 - 4 days after taking it. The info is on the website, the lying motherfuckers at NYT should investigate VAERS ID 1890705, if they have doubts. See below.

In fact, U.S. VAERS data from Dec. 14, 2020, to Dec. 10, 2021, for 5- to 11-year-olds show:
4,181 adverse events, including 80 rated as serious and 2 reported deaths. One death occurred in an 11-year-old girl from Georgia vaccinated Sept. 14, prior to the authorization of Pfizer’s COVID vaccine in the 5 to 11 age group.
The second death (VAERS I.D. 1890705) occurred in a 5-year-old girl who died four days after her first Pfizer shot.
U.S. VAERS data from Dec. 14, 2020, to Dec. 10, 2021, for 12- to 17-year-olds show:
24,893 adverse events, including 1,488 rated as serious and 33 reported deaths.
The most recent deaths involve a 13-year-old girl from Texas (VAERS I.D. 1913198) who died 31 days after receiving her COVID vaccine. According to her VAERS report, the girl received her first dose of Pfizer on Aug. 1.
Two weeks later, she complained of vague upper back pain and was diagnosed with a rare soft tissue cancer located on her heart despite having no previous medical history. Parents requested a VAERS report be filed in case her cancer was related to the vaccine. Her cancer and heart condition rapidly and progressively worsened and she died Dec 1.
61 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
571 reports of myocarditis and pericarditis (heart inflammation) with 561 cases attributed to Pfizer’s vaccine.
143 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to Dec. 10, 2021, for all age groups combined, show:
19% of deaths were related to cardiac disorders.
54% of those who died were male, 42% were female and the remaining death reports did not include the gender of the deceased.
The average age of death was 72.7.
As of Dec. 10, 4,584 pregnant women reported adverse events related to COVID vaccines, including 1,446 reports of miscarriage or premature birth.
Of the 3,285 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
791 reports of Guillain-Barré syndrome (GBS), with 42% of cases attributed to Pfizer, 29% to Moderna and 27% to J&J.
2,206 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
11,680 reports of blood clotting disorders in the U.S. Of those, 5,198 reports were attributed to Pfizer, 4,159 reports to Moderna and 2,275 reports to J&J.
3,405 cases of myocarditis and pericarditis with 2,118 cases attributed to Pfizer, 1,137 cases to Moderna and 140 cases to J&J’s COVID vaccine.
According to the latest data from the U.S. Vaccine Adverse Event Reporting System, there have been 20,836 reported adverse events following Pfizer’s COVID vaccine among 12 to 17-year-olds.
VAERS Underreporting Factor Affects Data
To compare the number of deaths from COVID illness against those who have died from the genetic therapy injection, we must address the known underreporting factor in VAERS. To date, the VAERS database is the only reporting system used by the CDC and FDA that is accessible to the public. According to VAERS, it:8
“… is a passive reporting system, meaning it relies on individuals to send in reports of their experiences. Anyone can submit a report to VAERS, including parents and patients.”
Additionally, it is the only area where the public, including doctors and other medical professionals, can voluntarily report vaccine adverse events, including death. According to VAERS,9 health care professionals are mandated by law to report serious injury adverse events that occur within a specified time period after the shot, and those events that are listed by the manufacturer as a contraindication to further doses.
However, the system only “encourages” providers to report events after vaccination whether the shot caused the event or not. In other words, the system depends on the health care professionals' knowledge that the VAERS system exists and their willingness to spend time filling out the document which asks for:10
While much of this information is necessary for data tracking, you can see how the time-consuming nature of filling out this form can easily become overwhelming when doctors have multiple patients with adverse events from the COVID-19 shots.11 Lack of knowledge of the system, and a growing physician shortage12 with subsequent lack of time have also likely contributed to the underreporting factor (URF).
In an early grant report submitted by the U.S. Department of Health and Human Services, which is part of the VAERS system, the writers admitted that:13
“Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.”
As of December 3, 2021, there were 946,461 adverse events and 19,886 deaths reported to the system.14 If only 1% of the events are reported, this translates to 94.64 million adverse events and 1.98 million deaths. To ascertain a better estimate of how many people have been injured from the current genetic injection, the issue of the URF was again addressed in a paper published in November 2021.15
The process for defining a new URF was published in a 62-page paper.16 Using an engineering analysis of the available data and judgment based on peer reviewed literature and expertise of the scientists, an underreporting factor of 41 was determined.
Researcher Steve Kirsch, recognized the gravity of the situation as it relates to the number of children who have died after taking the vaccine versus the number who have died from the illness. CDC data ending December 8, 2021,17 shows 757 children younger than 18 were listed as casualties of COVID-19.
He points out that many of these deaths, like those in adults, are likely children who died with COVID and not from COVID.18 However, to maintain simplicity, he used those numbers for comparison. Then, using data from VAERS ending December 3, 2021, he found 32 deaths from the vaccine.
Using the URF of 41, this suggests there have been 1,312 deaths that are likely to have been caused by the injection as compared to the 757 deaths the CDC records as having been caused by the illness. If you do the math, this means the shot has killed roughly 173% more children than the illness.
Using the same URF of 41 and the current data ending December 3, 2021, from OpenVAERS we can estimate there should have been 38,804,901 reports and 815,326 deaths caused by the injection. This is vitally important as the total number of deaths recorded for COVID-19 as of December 15, 2021. is 795,839.19 This means the shot has currently killed more children and adults than the virus. [MORE]
Offering an Allegedly Better Plantation w/Much Better Masters, Winsome Sears Wants Black Voters to Join the GOP. The Real Question is WTF Would Anyone Prefer Having a Master Over a World of Equals?
/
According to FUNKTIONARY:
Black Conservative - a lost sheep in master's clothing. A black conservative typically has nothing of his own to conserve with the exception of his or her own double-consciousness. So-called "Black Conservatives" dodge the reality of their folly and posit is that what they truly are conserving is traditional "values" as if values ever had anything whatsoever to do with morality or ethics. A black conservative unknowingly preserves the differential power-relations and dynamics between those of African descent he and their bosses, the overruling overclass elite. A black conservative is a turncoat made of wooly hair with no one to turn to tie because when it comes to empowering his own people, his master will turn to him say: "Get your hat, your robe and coat and leave—you're still just a nigger Clarence!" (See: Sambo, Nigger, Somnamnesiac, Values, Status Quo, Strawboss, Double Consciousness, Overclass, Uncle Tom. Status-Quoticians & Assimilationism)
The incoming lieutenant governor of Virginia was an unlikely candidate: a deeply conservative Black woman, and an immigrant, who supports Donald Trump. She will take office on Jan. 15, along with Governor-elect Glenn Youngkin.
The focus on Ms. Sears’s triumph, in news profiles and in the post-election crowing of conservative pundits, has been on the rare combination of her biography and politics: a Black woman, an immigrant and an emphatically conservative, Trump-boosting Republican.
“The message is important,” Ms. Sears, 57, said over a lunch of Jamaican oxtail with her transition team at a restaurant near the State Capitol. “But the messenger is equally important.”
This is the question that Ms. Sears embodies: whether she is a singular figure who won a surprise victory or the vanguard of a major political realignment, dissolving longtime realities of race and partisan identification. Democrats say there is little evidence for the latter, and that Ms. Sears won with typical Republican voters in an especially Republican year. But Ms. Sears insists that many Black and immigrant voters naturally side with Republicans on a variety of issues — and that some are starting to realize that.
“The only way to change things is to win elections,” she said. “And who better to help make that change but me? I look like the strategy.” [MORE]
Black conservatives call the Democratic party a plantation because it is - but so is the GOP. Elites maintain both plantations for all people. All statists (dems, GOP, libertarians, green, whatever believe in “authority”) want and need a master to obey. FUNKTIONARY explains,
Statism - the belief "citizens"' and "states" exist and the memetic thought patterns supporting such beliefs. 2) the religion of oppression and domination coupled with the science of exploitation and sociopathic control. 3) the opiate of the so-called Elites. 4) a philosophy that idealizes majority rule gang force (authority) over individual authenticity (autonomy). 5) servitude over liberty and statutes over humanity. [MORE]
Undeceiver Larken Rose explains, “There is a big difference between striving for a new, wiser, nobler master, and striving for a world of equals, where there are no masters and no slaves. Likewise, there is a big difference between a slave who believes in the principle of freedom, and a slave whose ultimate goal is to become the new master. And this is true, even if that slave truly intends to be a kind and generous master . . . As long as the people believe in the myth of “authority,” every downfall of one tyrant will be followed by the creation and growth of a new tyrant.“
Larken Rose further explains;
"Among those who vote Democrat or Republican – or for any other party – no one recognizes the underlying problem, and as a result, no one ever gets any closer to a solution. They remain slaves, because their thoughts and discussions are limited to the pointless question of who should be their master. They never consider – and dare not allow themselves to consider – the possibility that they should have no master at all. As a result, they focus entirely on political action of one kind or another, But the foundation of all political action is the belief in “authority,” which is the problem itself So the efforts of statists are, and always will be, doomed to fail.
Unfortunately, this is also true of the less mainstream, supposedly more pro-freedom “political movements,” including Constitutionalists, the Libertarian party, and others. As long as they think and act within the confines of the “government” game, their efforts are not only completely incapable of solving the problem but actually aggravate the problem by inadvertently legitimizing the system of domination and subjugation which wears the label of “government.”
The Rules of the Game
Even most people who claim to love liberty and to believe in “unalienable” rights allow the superstition of “authority” to drastically limit their effectiveness. Most of what such people do, in one way or another, consists of asking tyrants to change their “laws.” Whether activists campaign for or against a particular candidate, or lobby for or against a particular piece of “legislation,” they are merely reinforcing the assumption that obedience to authority is a moral imperative.
When activists try to convince politicians to decrease “taxes,” or repeal some “law,” those activists are implicitly admitting that they need permission from their masters in order to be free, And the man who “runs for office,” promising to fight for the people, is also implying that it is up to those in “government” to decide what the peasants will be allowed to do. As Daniel Webster put it, “There are men in all ages who mean to govern well, but they mean to govern; they promise to be good masters, but they mean to be masters.” Activists spend huge amounts of time, money and effort begging their masters to change their commands. Many even go out of their way to stress the fact that they are “working within the system,” and that they are not advocating anything “illegal.” This shows that, regardless of their displeasure with those in power, they still believe in the myth of “authority,” and will cooperate with “legal” injustice unless and until they can convince the masters to change the rules – to “legalize” justice. While the intended message of dissenters may be that they disapprove of what the masters are doing, the actual message that all political action sends to those in power is “We wish you would change your commands, but we will continue to obey whether you do or not.” The truth is, one who seeks to achieve freedom by petitioning those in power to give it to him has already failed, regardless of the response. To beg for the blessing of “authority” is to accept that the choice is the master’s alone to make, which means that the person is already, by definition, a slave.
One who begs for lower “taxes” is implicitly agreeing that it is up to the politicians how much a man may keep of what he has earned. One who begs the politicians not to disarm him (via “gun control”) is, by doing so, conceding that it is up to the master whether to let the man be armed or not. In fact, those who lobby for politicians to respect any of the people’s “unalienable rights” do not believe in unalienable rights at all. Rights which require “government” approval are not unalienable, and are not even rights. They are privileges, granted or withheld at the whim of the master. And those who hold positions of power know that they have nothing to fear from people who do nothing but pathetically beg for freedom and justice, However loudly the dissenters talk about “demanding” their rights, the message they actually send is this: “We agree, master, that it is up to you what we may and may not do.”
That underlying message can be seen in all sorts of activities mistakenly imagined to be forms of resistance. For example, people often engage in protests in front of “government” buildings, carrying signs, chanting slogans, sometimes even engaging in violence, to express their displeasure with what the masters are doing. However, even such “protests,” for the most part, do little more than reinforce authoritarianism. Marches, sit-ins, protests, and so on, are designed to send a message to the masters, the goal being to convince the masters to change their evil ways. But that message still implies that it is up to the masters what the people may do, which becomes a self-fulfilling prophecy: when the people feel beholden to an “authority,” they are beholden to an “authority.” Those in “government” derive all of their power from the fact that their subjects imagine them to have power.
Legitimizing Oppression
The harder people try to work within any political system to achieve freedom, the more they will reinforce, in their own minds and the minds of anyone watching, that the “system” is legitimate. Petitioning politicians to change their “laws” implies that those “laws” matter, and should be obeyed. Nothing better shows the power of the belief in “authority” than the spectacle of a hundred million people begging a few hundred politicians for lower “taxes.” If the people truly understood that the fruits of a man’s labor are his own, they would never engage in such lunacy; they would simply stop surrendering their property to the political parasites. Their trained-in desire to have the approval of “authority” creates in them a mindset not unlike the mindset of a slave: they literally feel bad about keeping their own money and making their own choices without
first getting the master’s permission to do so. Even when freedom is theirs for the taking, statists continue to grovel at the feet of megalomaniacs, begging for freedom, thus ensuring that they will never be free.
The truth is, one cannot believe in “authority” and be free, because accepting the myth of “government” is accepting one’s own obligation to obey a master, which means accepting one’s own enslavement. Sadly, many people believe that begging the master, via “political action,” is all they can do, So they forever engage in rituals which only legitimize the slave-master relationship, instead of simply disobeying the tyrants. The idea of disobeying “authority,” “breaking the law,” and being “criminals” is more disturbing to them than the idea of being a slave.
Those who want a significantly lower level of authoritarian control and coercion are sometimes accused of being “anti-government,” an allegation most vehemently deny, saying that they are not against “government” per se, but only want better “government.” But by their own words they are admitting that they do not believe in true freedom, but still believe in the Divine Right of Politicians and the idea that a ruling class can be a good and legitimate thing. Only someone who still feels an abiding obligation to obey the commands of politicians would want to avoid being labeled “anti-government.” Since “government” always consists of aggression and domination, one cannot be truly pro- freedom without being anti-”government.” The fact that so many activists reject that label (”anti-government”) shows how deeply ingrained the superstition of “authority” remains, even in the minds of those who imagine themselves to be ardent advocates of individual liberty.
(One particularly fascinating phenomenon is worth mentioning here. Outraged by authoritarian injustice, but still unwilling to give up the “authority” superstition in themselves, many in the growing freedom/militia/”patriot” movement continue to seek, or claim to have found, some “legal” remedy which will persuade tyrants to leave them in peace. Over the years, one theory after another has surfaced alleging the existence of some secret “government” form, or some “legal” trick, or some official procedure, which can free an individual from the control of “government.” Sadly, this demonstrates only that such people are still doing nothing more than looking for a way to get permission to be free. But the road to true freedom has never been, and will never be, a new political ritual, a new “legal” document or argument, or any other form of “political” action. The only road to true freedom is for the individual to let go of his own attachment to the superstition of “authority.”)"
Speaking for the Real Dems and the Willing-Slave Community, RecogNegro Michael Nutter Wants to Lock Up More Blacks [Racists Need NGHRS (and vice-versa) to maintain consensual Master/Servant Relations]
/From [HERE] When Larry Krasner, Philadelphia’s liberal district attorney, was asked this month about the city’s crime surge that includes an unprecedented 550 homicides this year, he said. “We don’t have a crisis of crime. We don’t have a crisis of violence.” Since then neuropeon and neuropean Dems and Republicans, who are obsessed with crime statistics in Black communities, have pretended to be super upset about it, as part of their general overall interest in the well being of Black people. Only a gullible NGHR would believe that racists have real concern about any Black community. Racist republicans and liberals always propagandize Black crime. Dr. Amos Wilson kept it real:
"Given the historical and contemporary virulence of White racism in America and the injustice toward Blacks that such racism engenders, the number of arrests, incarcerations, and in many instances, convictions of Black males should be viewed with a jaundiced eye. The willingness of White Americans to heavily tax themselves in order to finance accelerated and increased prison construction, rapidly expanding police forces and so-called criminal justice system personnel, burgeoning private police and security establishments; their willingness to finance the incarceration of a Black male prisoner upwards of $30,000 to $40,000 per year, in sharp contrast to their unwillingness to tax themselves to provide for the appropriate funding of the education of Black children and to commit themselves to the ending of racist employment practices; to provide adequate housing medical care, food and clothing; clearly implies that alleged Black male criminality plays a very important role in defining the collective White American ego and personality.”
Krasner, who is White, has been an ally of Black leaders pushing for changes to the criminal justice system, but SNAG Michael Nutter, a former Philadelphia mayor who is African American, erupted at Krasner, accusing him of dismissing the pain of Black residents who suffer from the violence while purporting to support them.
“It all goes back to supremacy, paternalism. 'I’m woke. I’m paying attention. I spend a lot of time with Black people. Some of my best friends … ’ All that bulls---," Nutter said in an interview. “And so you get a guy like Larry Krasner who is the great White hope and ‘I’m gonna ride in on a white horse with a white hat.’ ”

A safe-negro writer at the liberal Wash Post wrote, “It was a jarring rebuke of one Democrat by another. But it also laid bare a broader turbulence within the party and the progressive movement, as those pushing a message of racial equity sometimes do so with a zeal or tone that fails to resonate with portions of the Black or Latino communities. The dynamic is even more fraught when those ideas are championed by White leaders.'"
As opposed to a “black” leader like Nutter? lol, wtf makes Nutter black? Said negro writer sounds well trained by his elite masters, the same way Nutter was. Nutter, is a recognegro Sambo, basically a creation of elite whites, whose last poll numbers among Blacks in Phili were abysmal. Nutter functions as a proxymoron who speaks on behalf of his racist, moronic masters in the Democratic party. A major goal of racism white supremacy is to place Black men in greater confinement. Krasner, apparently is opposed to that but racists and NGHRS like Nutter are not.
Dr. Amos Wilson explains, "Alleged Black criminality, while evoking White American fear and loathing, reassures them of their vaunted self-worth, their assumed innately superior moral standing, of their self-congratulatory self-constraint in contrast with presumed Black American unworthiness, innate inferior moral standing, inherent criminality, lack of self-constraint and self-control.
White America's self-appreciation is enhanced as it insatiably feeds on overblown reports about Black criminality while denying its own incomparable criminal record, and its own racist-imperialist incubation and giving birth to the very same criminal forces which now threaten to destroy it.
Black criminals function as a negative reference group vital to maintaining the White American self-image. The Black criminal is used to support the White American community's self-serving, self-justifying judgments of itself. White America's preoccupation with Black criminality betrays its own need for reassurance; betrays its own basic insecurity regarding its projected moral purity. Consequently, the higher the incidence of reported Black criminality, the more exceptionally righteous White America feels itself to be. The more righteous it feels itself to be the more intensely and guiltlessly it promulgates and justifies its domination and exploitation of African peoples at home and abroad. [MORE]
Alleged Black criminality plays a very important role in defining the collective White American ego and personality. [MORE] Racists project criminality upon Blacks in order to treat Blacks criminally and to simultaneously empower themselves. Wilson states, such maneuvers are necessary in order to justify racist White American community's repression of African Americans and psychodynamically defend the collective White American ego complex. [MORE]
FUNKTIONARY defines:
Negro - a man or woman of Afrikan descent living in pathological mental state of cultural abstinence and historical amnesia— one who wants to impress his or her oppressor while ignoring the effects and plight that his or her accommodationist posture inures. 2) a Hanky-head. 3) an indigenous-to-the-land (American) Afrikan who does everything in his or her power to suppress or pretend that he or she is other than someone of recent Afrikan descent. 4) ethnicity-denying, assimilated and confused Afrikans indigenous to America. 5) one who truly believes he or she is white American—masquerading in black face. Mirror, mirror on the wall, who's a Negro after all? (See: Snigger, Rentellectual, McNegro & Negropolitan)

Doctors Release Public Statement: COVID Poses a Negligible Risk of Permanent Harm to Otherwise Healthy Persons, No Empirical Evidence Exists to Show Healthy Asymptomatic People Spread It
/
Summary
This expert statement makes the case that
the WHO’s act of declaring COVID-19 a “pandemic” was unjustified;
COVID-19 poses a negligible risk of permanent harm to otherwise healthy persons, particularly those of young age;
no empirical evidence exists to support the use of masks, social distancing, or lock-downs to prevent the spread of COVID;
empirical evidence does exist to show that healthy people do not infect others with COVID;
lock-downs, school closures and other scientifically baseless ‘pandemic control measures’ have devastating effects on the mental health of our children.
Measures such as lock-downs, mask mandates, and school closures are therefore unsupportable and should be revoked.
From Michael Palmer MD and Sucharit Bhakdi MD [PDF]
1. The misconception of the “COVID-19 emergency”
The WHO issued its declaration of a “pandemic” on March 11th, 2020. Considering that less than two weeks before that date the number of “cases” reported worldwide had been only 80,000 [1], this declaration was strangely premature. However, this low case number is not the only thing that was amiss with this “emergency.”
1.1. The WHO’s criteria for calling a “pandemic” are flawed
British Medical Journal editor Peter Doshi has pointed out that, shortly before Swine Flu was declared a “pandemic” in 2009, the WHO had redefined its criteria for making such a declaration [2]. According to Doshi, as of 2003 the now defunct WHO Pandemic Preparedness homepage had contained the following statement:
An influenza pandemic occurs when a new influenza virus appears against which the human population has no immunity, resulting in several simultaneous epidemics worldwide with enormous numbers of deaths and illness.
A definition that includes “enormous numbers of death and illness” is certainly in keeping with the general understanding of the term “pandemic,” considering that it is commonly used in connection with the “Black Death” of the Middle Ages or with the Spanish Flu of 1918. However, the WHO’s revised definition from 2009 does not contain any reference to deaths or disease severity. As of that year, the same WHO web page merely stated:
An influenza pandemic may occur when a new influenza virus appears against which the human population has no immunity.
Nor do death or clinical disease severity receive any mention in the more detailed definition given by the WHO’s 2009 guidance document on influenza epidemics, which is currently still available [3]. Accordingly, pursuant to these guidelines, any new strain of influenza could be declared a “pandemic,” whether or not it results in significant surplus mortality and morbidity.
Considering the far-reaching and detrimental consequences for commerce, international travel etc., it should go without saying that declaring a pandemic is disproportionate and unjustified when the disease in question is merely widespread but not severe. Exactly this kind of malfeasance, however, has occurred in the case of COVID-19: a pandemic was declared by the WHO, and subsequently by the governments of the world, without regard for clinical severity.

1.2. All-cause mortality soared only shortly after the declaration of the COVID-19 “pandemic,” not before
Figure 1: All-cause mortality in New York city and in Texas, before and after the declaration of the COVID-19 “pandemic” by the WHO (red vertical line). A sharp yet short-lived spike occurred in New York City immediately after the declaration, whereas no such event manifested itself in Texas. Before the declaration, all-cause mortality for the winter 2019/20 had been tracking significantly lower than two years before; the higher mortality rate during that previous winter season was due to a worldwide outbreak of influenza that was not declared a pandemic. Graphics taken from Figures 8 and 10 in [4].
Rancourt has examined the correlation in time between the WHO’s declaration of the “pandemic” and all-cause mortality in various jurisdictions [4]. Immediately after the declaration, there occurred a sharp peak in all-cause mortality in some jurisdictions, but not in others; this discrepancy is illustrated in Figure 1 for New York City and Texas.
Common sense and historic precedents suggest that a deadly virus pandemic would not respect international or state borders. Furthermore, if the virus had indeed been both deadly and truly novel, the wave of deaths in New York should not have subsided within such a short time period as is apparent from Figure 1. Thus, as Rancourt convincingly argues, any peaks in mortality were most likely caused by government malfeasance, which led to consequences such as the rapid spread of the infection in senior homes. In the case of New York, this has led to the filing of criminal complaints against former governor Andrew Cuomo.
1.3. Mortality due to COVID-19 is very low except in the frail and elderly
In the vast majority of people (≥ 99.8% globally), an infection with SARS-CoV-2, the causative agent of COVID-19, is non-lethal [5–7]. It is typically a mild to moderately severe illness with a case fatality rate similar to that of influenza (see again Figure 1 for context). The relationship of COVID mortality with age is illustrated in Figure 2. Panel A very clearly shows that mortality is vanishingly small in the young and middle-aged. Moreover, even among the elderly, almost all fatal cases occur in people with co-morbidities. In Italy, the average age at the time of death was above 80 years, and only 0.8% of all fatal cases suffered from none of the 10 most common co-morbidities [8]. University of Hamburg forensic pathologist Prof. Klaus Püschel reviewed over 100 autopsies on patients at his institution whose deaths had been ascribed to COVID-19, and he concluded that not one of them had died due to COVID alone [9].
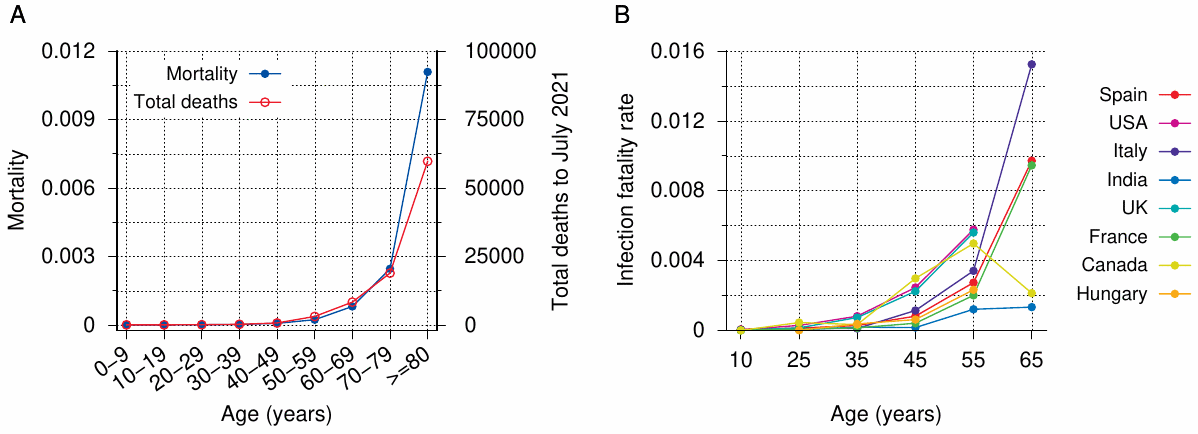
Figure 2: COVID mortality, number of cases, and infection fatality rate by age group. A: Total cases reported to the Robert Koch Institute as of July 13þ, 2021, and mortality per age group, based on 2018 census numbers [10]. B: Infection fatality rates by age in various countries. Adapted from Figure 3 in [11].
The collective findings can be summarized as follows: in otherwise healthy persons of all ages, COVID-19 poses a negligible risk of death or of severe disease with irreversible harm.
1.4. The misconception of the “pandemic” was implanted and perpetuated with inappropriate testing practices
From the very beginning, the number of COVID “cases” was artificially inflated by the inappropriate use of the PCR test. There are two key aspects to this misuse of the technique:
the calibration of the method is inadequate; in particular, the number of amplification cycles is excessive;
the application of the PCR test to healthy (“asymptomatic”) people, for example in connection with travel. This could not but generate a large number of false positive test results, which were then elevated to “cases.”
For further detail pertaining to this question, please refer to Prof. Ulrike Kämmerer’s separately submitted PCR expertise.
1.5. Flattening which curve?
When the first restrictions such as masks, “social distancing,” and lock-downs were imposed on the public, they were justified with the purported need to “flatten the curve,” that is, to slow down the spread of the virus so as to distribute clinically severe cases in time and thereby avoid the overload of hospitals with grave COVID cases. Media outlets such as the Canadian CBC propped up this narrative with invented stories about overflowing hospitals; see for example the fraudulent CBC story about triage of patients in the parking lot of the hospital in Steinbach, Manitoba—a reporter from another media outlet who investigate on-site found both the parking lot and the hallways of the hospital deserted [12].
In the real world, emergency room visits and hospital admissions declined after the declaration of the “pandemic;” this was consistently reported from various countries [13–17]. The reason for the decline was likely a general reluctance in the population to seek medical assistance, for fear of being infected with the supposedly deadly virus at the hospital. The decline was not offset by any proportional numbers of actual severe COVID cases. Thus, the need for “flattening the curve,” and with it that for imposing the very harsh and oppressive “emergency” measures, never existed.
2. On the necessity and effectiveness of the restrictions imposed by the governments
2.1. Do lock-downs and other restrictions reduce COVID mortality?
Reports like the one by Püschel (see Section 1.3) make it clear that COVID mortality statistics cannot be trusted. Püschel’s use of autopsies is of course the correct approach; in order to understand the seriousness of a novel pathogen, it would be essential to perform autopsies on as large a scale as possible. However, in general, autopsies were rarely performed and discouraged by the authorities worldwide. In their literature review entitled No Autopsies on COVID-19 Deaths: A Missed Opportunity and the Lockdown of Science, Salerno et al. observe [18]:
Despite the increasing number of published studies on COVID-19, in all the examined studies the lack of a well-defined pathophysiology of death among patients who died following COVID-19 infection is evident. Autopsy should be considered mandatory to define the exact cause of death … Only 7 papers reported histological investigations. Nevertheless, only two complete autopsies are described and the cause of death was listed as COVID-19 in only one of them.
The lack of rigorous standards for determining the causes of death in diagnosed cases of the infection has produced a very large spread in the COVID mortality rates reported by different countries (Figure 3A). While some variation between countries must be expected, it surely is difficult to believe that the mortality in France, whose healthcare system is considered of very high quality, should be twenty times higher than in Iceland, or that Belgium should have five times more deaths per capita than Denmark.
The distortion apparent in these numbers makes it impossible to place any trust into those in panel B of the same figure. This graph shows the correlation—or rather, the lack thereof—between a “stringency index,” which summarizes the rigour of the lock-down and other measures imposed by national governments, and the reported COVID deaths. In this sample of 31 European countries (which includes the 16 countries represented in panel A), the correlation is very low, with an R2 value of only 0.02 (and a positive slope of the linear regression line). In other words, the quality of the mortality data is so low as to render the task of discerning any correlation between the stringency of lock-down measures and COVID mortality hopeless. In view of this deplorable quality of the raw data, it is unsurprising that proper epidemiological studies, too, fail to detect any benefits of more restrictive interventions [19,20].
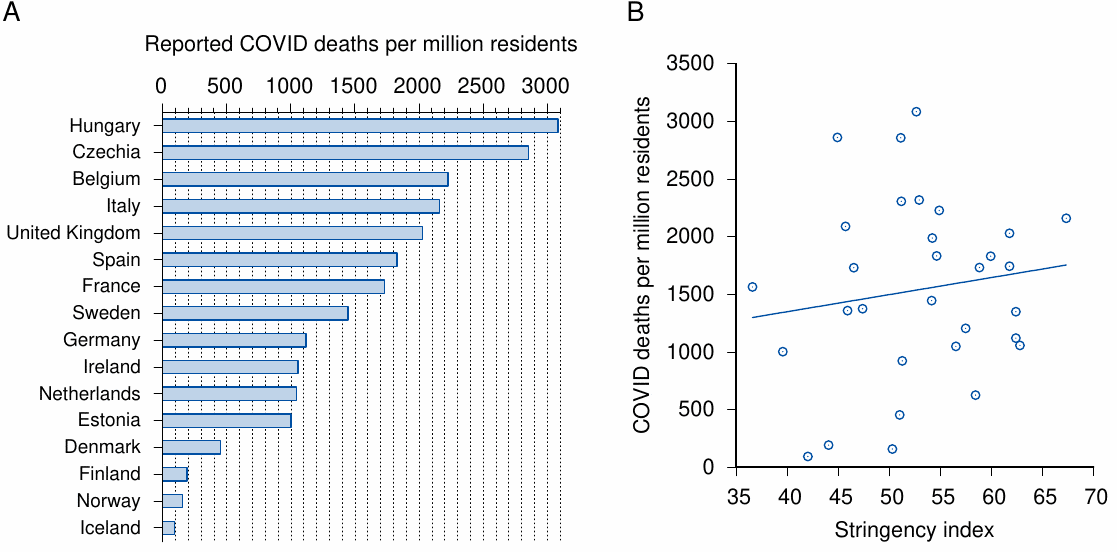
Figure 3: COVID mortality and stringency of government responses across European countries. A: COVID mortality per million residents in 16 European countries. B: COVID mortality vs. stringency of government response for 31 European countries. The linear regression line shown has an R2 value of 0.02. Mortality data from [21] as of September 16th, 2021; response stringency index from [22] as of September 23rd, 2021.
2.2. Lock-downs and overall mortality
We just saw that it is impossible to statistically detect any benefit of lock-downs and other mandates and restrictions imposed on the populace. The only recourse is to look at excess overall mortality during the “pandemic.” An instructive example is the comparison of three European countries provided by Kowall et al. [23]. In contrast to both Spain and Germany, Sweden never imposed any school closures or other hard “lock-down” measures, yet its standard mortality rate is unremarkable in comparison with these two other countries (see Figure 4). Kowall et al. also review possible causes for the observed excess mortalities in Spain and in Sweden, without however offering a definite conclusion regarding role of the lock-down measures. Obviously, no certain conclusions are possible in this regard based on the limited information available.
2.3. Do masks work?
A meta-analysis of 15 clinical studies by an international consortium of epidemiologists and infectious disease specialists offers the following conclusions [24]:
Compared to no masks there was no reduction of influenza-like illness (ILI) cases … or influenza … for masks in the general population, nor in healthcare workers … There was no difference between surgical masks and N95 respirators … Harms were poorly reported and limited to discomfort with lower compliance.
If no effect on disease transmission can be demonstrated even with the use of proper surgical or N95 masks, then surely the notion that those fashionable cloth masks will provide any benefit is fanciful. In conclusion, the evidence shows that masks don’t work.
We should note that influenza viruses and coronaviruses differ in some aspects of their biology from each other and from other “influenza-like” viral pathogens. However, all of these viruses are equivalent when it comes to airborne transmission—the viruses are exhaled with micro-droplets, which may or may not be inhaled by another person. The question as to whether a mask reduces transmission comes down simply to its ability to stop these micro-droplets, regardless of the identity of their viral cargo. Thus, the findings reported by Jefferson et al. are valid for COVID-19 as well.

Figure 4: Weekly standardized mortality ratio (SMR) by calendar week in Spain, Germany and Sweden (with consideration of life expectancy). Adapted from Figure 3 in [23].
A recent “cluster-randomized trial” conducted in Bangladesh claims to finally have unearthed the missing evidence to support the effectiveness of masks. The study was predictably covered with great fanfare in the mainstream press; it does, however, not stand up to scrutiny. The diagnostic method used in this study was an IgG antibody test, which is not suitable for diagnosing current or recent infections. Moreover, the study reports that the proportion of those with symptoms and a positive antibody test among the masked group was 0.76%, whereas in the unmasked group it was 0.68%. Passing off a reduction of 0.08% in an irrelevant diagnostic parameter as proof that masks reduce acute COVID infections is evidence not of mask effectiveness but of scientific incompetence, or worse. Rancourt [25] further dissects the many flaws of the study by Abaluck et al.
2.4. Is COVID likely to be transmitted outdoors?
It is well accepted that the risk of airborne transmission of infections is highest in indoor spaces that have limited ventilation with outdoor air [26–28]. Unlike the air in enclosed spaces, outdoor air will not stagnate or be recirculated, and it generally has a lower relative humidity, which will cause more rapid evaporation of exhaled micro-droplets. In addition, outdoors there is a higher level of ultraviolet radiation, which inactivates airborne microbes. Single-stranded RNA viruses such as SARS-CoV-2 are particularly sensitive to UV irradiation. Therefore, while to my knowledge no hard evidence exists to completely rule out outdoors transmission of COVID, the likelihood is certainly far lower than indoors. Thus, confining healthy people to their homes in order to ‘flatten the curve’ or ‘stop the spread of COVID’ is disproportionate and unreasonable.
2.5. Can clinically healthy people transmit COVID?
A subtext of the imposition of sweeping masking, distancing, or lock-down mandates on clinically healthy people is the idea of “asymptomatic spread”—persons who have been infected, but who show no signs of it other than a positive PCR test, are assumed to transmit this infection to other susceptible individuals. If we accept the idea of such asymptomatic spread, then the above drastic measures might indeed appear reasonable means for protecting those at risk.
It has, however, been unambiguously determined that such asymptomatic transmission is not relevant in practice. In a large-scale study, which involved almost 10 million Chinese residents, no new infections could be traced to persons that had tested positive for SARS-CoV-2 by PCR, but who did not exhibit any other signs of infection [29]. This agrees with several studies which compared PCR to virus isolation in cell culture among patients with acute COVID-19 disease. In all cases, growth of the virus in cell culture ceased as symptoms subsided, whereas PCR remained positive for weeks or months afterwards [30,31]. It was accordingly proposed to use cell culture rather than PCR to assess infectiousness and to determine the duration of isolation [31].
These findings indicate that restricting contact of persons at risk with those who show, or very recently showed, symptoms of acute respiratory disease would be effective and sufficient as a protective measure. Indiscriminately restricting the movements of persons who are not themselves at risk of severe disease, or of those who are currently asymptomatic is not required to achieve such protection.
2.6. COVID-19 can be treated effectively
A convergence of evidence indicates that early treatment of COVID-19 with existing drugs reduces hospitalisation and mortality by ~85% and 75%, respectively [32–36]. These treatment protocols include many tried and true antiviral, antiinflammatory, and anticoagulant medications, as well as monoclonal antibodies, zinc, and vitamins C and D. Two of the safest and most effective drugs for early treatment are ivermectin and hydroxychloroquine. Ivermectin, in particular, is generally considered so safe that it is often prescribed even in scabies, an unpleasant but harmless parasite disease of the skin that can be cured with topical treatment. It’s very strong inhibition of SARS-CoV-2 in vitro [37] can account for its observed clinical effectiveness.
The current restrictions and obstacles imposed by the WHO [38] and other authorities worldwide regarding the availability and distribution of these proven and safe drugs are scientifically and medically unjustifiable; they are simply more evidence of deliberate government malfeasance.
3. Lock-downs and children’s mental health
Kowalyshyn et al. have reviewed the literature on the effects of school closures, social distancing etc. on child mental health [39]. The authors note a very substantial increase of child suicides and suicide attempts in the year 2020. Here is the evidence. The Children’s Hospital of McMaster University in Hamilton, Ontario, reported an almost 300% increase in youth suicide attempts between October 2020 and January 2021, compared to the same time period one year before. The city of Pima, Arizona reported a 67% increase in child suicides during the 2020 lock-down, and Boston Children’s Hospital reported a 47% increase in children hospitalized for suicide attempts and suicide ideation between July and October 2020 compared to the same period in 2019.
These harrowing findings make it clear that the supposed pandemic control measures are not only unfit for their declared purpose, but that they are doing real harm to the health and sometimes even the lives of our children. Any such measures must be stopped immediately.
References
Cucinotta, D. and Vanelli, M. (2020) WHO Declares COVID-19 a Pandemic. Acta biomed91:157-160
Doshi, P. (2011) The elusive definition of pandemic influenza. Bull. World Health Organ.89:532-8
Anonymous, (2009) Pandemic Influenza Preparedness and Response: A WHO Guidance Document.
Rancourt, D. (2020) All-cause mortality during COVID-19: No plague and a likely signature of mass homicide by government response. (Unknown journal) (preprint)
Ioannidis, J.P.A. (2020) Global perspective of COVID‐19 epidemiology for a full‐cycle pandemic. Eur. J. Clin. Invest. 50 (preprint)
Ioannidis, J.P.A. (2021) Reconciling estimates of global spread and infection fatality rates of COVID‐19: An overview of systematic evaluations. Eur. J. Clin. Invest. 5:e133554
Ioannidis, J.P.A. (2020) Infection fatality rate of COVID-19 inferred from seroprevalence data. Bull. World Health Organ. p. BLT.20.265892
Anonymous, (2020) Report sulle caratteristiche dei pazienti deceduti positivi a COVID-19 in Italia. Il presente report è basato sui dati aggiornati al 17 Marzo 2020.
Pueschel, K. (2020) Forensic Pathologist: No One in Hamburg Has Died of COVID-19 Alone.
Anonymous, (2020) Bevölkerung nach Altersgruppen und Geschlecht.
Axfors, C. and Ioannidis, J.P. (2021) Infection fatality rate of COVID-19 in community-dwelling populations with emphasis on the elderly: An overview. medRxiv (preprint)
Bexte, K. (2020) CBC says this Manitoba hospital is OVERWHELMED by COVID—is it really? Keean Bexte investigates.
Hartnett, K.P. et al. (2020) Impact of the COVID-19 Pandemic on Emergency Department Visits — United States, January 1, 2019-May 30, 2020. MMWR. Morbidity and mortality weekly report 69:699-704
Kruizinga, M.D. et al. (2021) The impact of lockdown on pediatric ED visits and hospital admissions during the COVID19 pandemic: a multicenter analysis and review of the literature. Eur. J. Pediatr. 180:2271-2279
Kuitunen, I. et al. (2020) The effect of national lockdown due to COVID-19 on emergency department visits. Scand. J. Trauma Resusc. Emerg. Med. 28:114
Ojetti, V. et al. (2020) Non-COVID Diseases during the Pandemic: Where Have All Other Emergencies Gone?. Medicina 56 (preprint)
Rennert-May, E. et al. (2021) The impact of COVID-19 on hospital admissions and emergency department visits: A population-based study. PLoS One 16:e0252441
Salerno, M. et al. (2020) No Autopsies on COVID-19 Deaths: A Missed Opportunity and the Lockdown of Science. J. Clin. Med. 9 (preprint)
Bendavid, E. et al. (2021) Assessing mandatory stay‐at‐home and business closure effects on the spread of COVID‐19. Eur. J. Clin. Invest. 51 (preprint)
De Larochelambert, Q. et al. (2020) Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation. Frontiers in public health 8 (preprint)
Anonymous, (2021) Incidence of coronavirus (COVID-19) deaths in the European Economic Area and the United Kingdom as of September 19, 2021, by country.
Anonymous, (0) COVID-19 Government Response Tracker.
Kowall, B. et al. (2021) Excess mortality due to Covid-19? A comparison of total mortality in 2020 with total mortality in 2016 to 2019 in Germany, Sweden and Spain. PLoS One16:e0255540
Jefferson, T. et al. (2020) Physical interventions to interrupt or reduce the spread of respiratory viruses. Part 1—Face masks, eye protection and person distancing: systematic review and meta-analysis. medRxiv (preprint)
Rancourt, D. (2021) Do Face Masks Reduce COVID-19 Spread in Bangladesh? Are the Abaluck et al. Results Reliable?.
Knibbs, L.D. et al. (2011) Room ventilation and the risk of airborne infection transmission in 3 health care settings within a large teaching hospital. American journal of infection control 39:866-72
Morawska, L. and Milton, D.K. (2020) It Is Time to Address Airborne Transmission of Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 71:2311-2313
de Man, P. et al. (2021) Outbreak of Coronavirus Disease 2019 (COVID-19) in a Nursing Home Associated With Aerosol Transmission as a Result of Inadequate Ventilation. Clin. Infect. Dis. 73:170-171
Cao, S. et al. (2020) Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat. Commun. 11:5917
Wölfel, R. et al. (2020) Virological assessment of hospitalized patients with COVID-2019. Nature 581:465-469
Basile, K. et al. (2020) Cell-based culture of SARS-CoV-2 informs infectivity and safe de-isolation assessments during COVID-19. Clin. Infect. Dis. (preprint)
Orient, J. et al. (2020) A Guide to Home-Based COVID Treatment.
McCullough, P.A. et al. (2020) Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19). Reviews in cardiovascular medicine 21:517-530
Procter, B.C. et al. (2021) Early Ambulatory Multidrug Therapy Reduces Hospitalization and Death in High-Risk Patients with SARS-CoV-2 (COVID-19). International journal of innovative research in medical science 6:219-221
McCullough, P.A. et al. (2021) Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection. Am. J. Med. 134:16-22
Anonymous, (2020) Real-time database and meta analysis of 588 COVID-19 studies.
Caly, L. et al. (2020) The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Res. 178:104787
Anonymous, (2021) WHO advises that ivermectin only be used to treat COVID-19 within clinical trials.
Kowalyshyn, J. and Alexander, P.E. (2021) Deaths of Despair: Child suicde evidence package.
Parroting his Master’s Dogma, Halfrocentric Clone Kareem Abdul-Jabber Criticizes Lebron for Not Promoting Experimental, Useless COVID Injections that Kill/Harm People and are Shielded from Liability
/
“Smile Negro And Grin—while I put it in.” FUCK A SNAG & NEVER TRUST A COIN-OPERATED CLONE. KAREEM WOULD SELL OUT HIS PEOPLE JUST TO GET A PAT ON THE HEAD FROM HIS RACIST MASTERS. SHADOWBOX ANOTHER BLACK MAN FOR NOT ADVOCATING THE DEATH OF HIS OWN PEOPLE? MF SAMBO TRAITOR.
“KAREEM GONE.” From [HERE] NBA legend Kareem Abdul-Jabbar asked LeBron James to make his stance on the COVID-19 vaccine clear due to his influence on the African-American community.
“I don’t talk about other people and what they should do. We’re talking about individual bodies. We’re not talking about something political or racism or police brutality. I don’t think I personally should get involved in what other people do for their bodies and livelihoods … I know what I did for me and my family … But as far as speaking for everybody and their individualities and things they want to do, that’s not my job,” James said in September.
Kareem penned an article, parroting his masters about how COVID-19 has disproportionately impacted the African-American community, at least in part due to their distrust of vaccines.

This past weekend, James posted the above meme on his Instagram account, comparing COVID-19 to the flu. Apparently, Kareem’s masters Big Tech, Big Pharma, Authority [aka Uncle Brother, Crimeth Inc., Doggy] and their Dependent Media needed what they think is an influential Black spokesperson to censor Lebron, so they trotted Kareem out to do so. The usual authoritarian playbook calls for bignorant, propaghandi to attack the person’s character and never to actually discuss COVID injection facts and research in contention. That is, Kareem didn’t refute Lebron’s contention that in reality COVID is like the Flu or an overblown plandemic. Rather, Kareem just shadowboxed Lebron for his white masters. Well done, negro. This has been the pattern with any celebrity figure, white or Black who dares to criticize or remain neutral to Big Pharma’s deadly COVID injections.
Big up to BronBron for taking a risk against the vested interests. Contrary to SNigger Kareem, in reality:
All-cause mortality soared only shortly after the declaration of the COVID-19 “pandemic,” not before
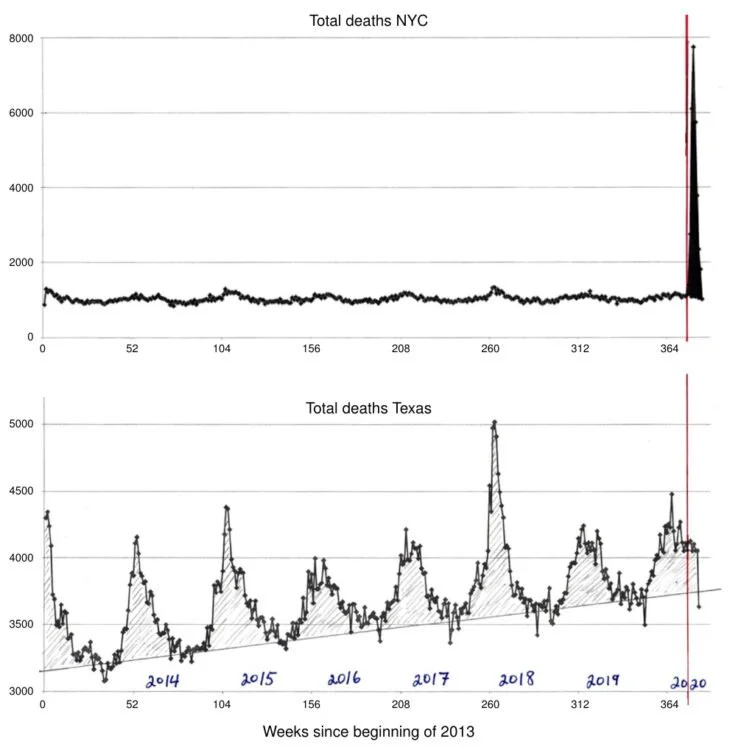
Figure 1: All-cause mortality in New York city and in Texas, before and after the declaration of the COVID-19 “pandemic” by the WHO (red vertical line). A sharp yet short-lived spike occurred in New York City immediately after the declaration, whereas no such event manifested itself in Texas. Before the declaration, all-cause mortality for the winter 2019/20 had been tracking significantly lower than two years before; the higher mortality rate during that previous winter season was due to a worldwide outbreak of influenza that was not declared a pandemic. Graphics taken from Figures 8 and 10 in [4].
Rancourt has examined the correlation in time between the WHO’s declaration of the “pandemic” and all-cause mortality in various jurisdictions [4]. Immediately after the declaration, there occurred a sharp peak in all-cause mortality in some jurisdictions, but not in others; this discrepancy is illustrated in Figure 1 for New York City and Texas.
Common sense and historic precedents suggest that a deadly virus pandemic would not respect international or state borders. Furthermore, if the virus had indeed been both deadly and truly novel, the wave of deaths in New York should not have subsided within such a short time period as is apparent from Figure 1. Thus, as Rancourt convincingly argues, any peaks in mortality were most likely caused by government malfeasance, which led to consequences such as the rapid spread of the infection in senior homes. In the case of New York, this has led to the filing of criminal complaints against former governor Andrew Cuomo.
Mortality due to COVID-19 is very low except in the frail and elderly
In the vast majority of people (≥ 99.8% globally), an infection with SARS-CoV-2, the causative agent of COVID-19, is non-lethal [5–7]. It is typically a mild to moderately severe illness with a case fatality rate similar to that of influenza (see again Figure 1 for context). The relationship of COVID mortality with age is illustrated in Figure 2. Panel A very clearly shows that mortality is vanishingly small in the young and middle-aged. Moreover, even among the elderly, almost all fatal cases occur in people with co-morbidities. In Italy, the average age at the time of death was above 80 years, and only 0.8% of all fatal cases suffered from none of the 10 most common co-morbidities [8]. University of Hamburg forensic pathologist Prof. Klaus Püschel reviewed over 100 autopsies on patients at his institution whose deaths had been ascribed to COVID-19, and he concluded that not one of them had died due to COVID alone [9].

Figure 2: COVID mortality, number of cases, and infection fatality rate by age group. A: Total cases reported to the Robert Koch Institute as of July 13þ, 2021, and mortality per age group, based on 2018 census numbers [10]. B: Infection fatality rates by age in various countries. Adapted from Figure 3 in [11].
The collective findings can be summarized as follows: in otherwise healthy persons of all ages, COVID-19 poses a negligible risk of death or of severe disease with irreversible harm.
The misconception of the “pandemic” was implanted and perpetuated with inappropriate testing practices
From the very beginning, the number of COVID “cases” was artificially inflated by the inappropriate use of the PCR test. There are two key aspects to this misuse of the technique:
the calibration of the method is inadequate; in particular, the number of amplification cycles is excessive;
the application of the PCR test to healthy (“asymptomatic”) people, for example in connection with travel. This could not but generate a large number of false positive test results, which were then elevated to “cases.” [MORE]
According to FUNKTIONARY:
SNAGs - $nitch-ass Negroes Aiding Governments. 2) COINTEL-BROs. 3) Smile Negro And Grin—while I put it in. SNAGs are coin-operated piece-activist sniggering infiltraitors from the native Black American community. SNAGs are on the stroll, exacting Black life as the toll, while klandestinely on the rogue "government" payroll. Dumb-ditty dumb where the hell do these sorry-ass sellout Negroes come from? When you see them, go and give them some—or at least a piece of your mind. It's easy to heckle and hyde, but why do we seem to always let self-hating sucker-perpetrating Negroes electric slide? SNAGs are Negroes who run from the fabric, the very essence of their Afrikan heritage struggle, culture and consciousness, and run to support the psychopathological dominant minority elite European global racist-supremacist mindset and Agenda along with its narcissistic projections and population control objectives (genocide and eugenics). The more you pull at a snag, the more problems it causes—hence, you have to cut it off from the garment so it will cease causing constraint and strain on the integrity of the fabric of Afrikan consciousness and liberation. Don't just run them off, cut them off. SNAGs get dealt with! SNAG's are responsible for facilitating agents of various "government intelligence" operations in successfully accomplishing the "wet jobs" (assassinations) and downfall of some of our most cherished leaders, luminary thinkers, uncompromising revolutionaries and lovers of justice for all humanity. SNAGs come in all shapes, colors, sizes and forms within the Black American community but they all share one common thread—self-hatred. Some of the less known but high-exposure SNAGs were Alex Haley (who covertly worked his roots on Malcolm X), Ernest Withers (civil rights photographer and FBI informant), and Justice Thurgood Marshall (also snitching and informing on the Right-Reverend Martin L. King, Jr.), not to mention another "Reverend" from Memphis, TN who was involved (along with Jesse Jackson) in the orchestration of King's assassination. SNAGs have also been known to be complicit in both successful and botched assassination schemes plotted and executed by the shadowy characters within and behind the veil of the Corporate State and its wet-works black operations spy agencies. (See: COINTELPRO, FBI, CIA, Manhood, Snigger, Sigma Pi Phi, Coin-Operated, Racism White Supremacy, HO-Method, Infiltraitors, Wet Jobs & Piece-Activist) [MORE]
“Comply or Go To Jail" [the False Choice Offered in the Free Range Prison]: Liberal New Yorkers Use the NYPD to Enforce Their New Vax Papers Law to Break Up a Child's Birthday Party at a Restaurant
/
The video captured Monday shows a group of at least a dozen NYPD vaccine enforcers surround a child and his friends at a restaurant, demanding to see their vaccine passports. “If you don’t have it, you’re going to have to leave,” an officer tells the unmasked child, who proceeds to cry. When it was apparent none of them had their vaccine papers, the cops began breaking up the gathering. [MORE]
Dr Peter McCullough says COVID Injections are the ‘most dangerous biological medicinal product rollout in human history' and provides Detailed evidence of the devastating damage COVID Jabs can do
/From [HERE] At a recent online symposium on covid science that was organized by Doctors for COVID Ethics, the most detailed evidence yet against Wuhan coronavirus (Covid-19) “vaccination” was presented for the world’s consideration.
This international group, which has long opposed the mass rollout of Fauci Flu shots, argued that the human immune system, provoked by the injections, could end up attacking its own tissues (autoimmune disease) when it detects the presence of synthetic spike proteins.
Untold thousands of deaths have already occurred from this, though most of them never make it into the government databases. Numerous presenters, including Dr. Peter McCullough, who has also long stood against the injections, revealed scientific evidence to support these and other claims.
McCullough, by the way, has actually come out to say that covid “vaccines” are the “most dangerous biological medicinal product rollout in human history.” He remains one of the most vocal opponents to the current agenda.
German pathologist and professor Dr. Arne Burkhardt, who has more than 40 years of experience in the field, also presented at the symposium. He conducted his own research on the tissues and organs from 15 different patients where a post-mortem had been performed.
Eight of the bodies were women and seven were men, all between the ages of 28 and 95. Each of these individuals died between seven days and six months post-injection.
What Burkhardt found is that in nearly every case, the jabs caused the individuals’ bodies to self-destruct. A specific type of immune cell called a lymphocyte was found to have invaded various parts of the body, eventually causing early death.
Burkhardt presented slides showing that lymphocytes had infiltrated the heart muscle in particular, causing systemic inflammation. The resulting lesions were small and probably overlooked, “but the destruction of just a few muscle cells may have a devastating effect,” he warned.
“If the inflammatory infiltration is found where the impulse for the contraction of the heart is given, this may lead to heart failure,” he further said.
It was also discovered that a lymphocyte invasion occurred in other vital organs such as the liver, kidneys, uterus, brain, thyroid and skin, all of which showed signs of autoimmune damage.
How much mRNA poison can the body handle before it goes kaput?
Canadian microbiologist and professor Dr. Michael Palmer summed up Burkhardt’s presentation by explaining that anyone with honest medical training will clearly see “just how devastating the effect of these vaccines can be, at least in those who die after the vaccination.”
“We also now know why the authorities were very hesitant to have autopsies performed on such victims,” Palmer added.
As to why some people are not suffering such an extreme fate post-injection, Palmer warned that the total lifetime dose of messenger RNA toxins is limited, suggesting that it varies from person to person.
Due to a lack of experimental data, it is unknown what these thresholds are. And according to Palmer, this is “one of the great scandals of these vaccines, that no proper toxicity studies have been carried out.”
We do know from animal studies that the contents of the jabs do not remain at the site of injection. They circulate throughout the entire body, combining with receptors and lining blood vessels, which in many people causes clotting and excessive bleeding.
The long-term risks of this are what will really be telling once the contents of the jabs really make their way throughout people’s bodies over the long haul. Widespread death from seemingly no specific cause is likely to occur in the coming months and years.
A Number of Medical Experts, Scientists and Published Studies Prove that Endless Boosters Destroy Immune Function and the Higher the Vax rate in a Given area, the Higher the COVID "case rate"
/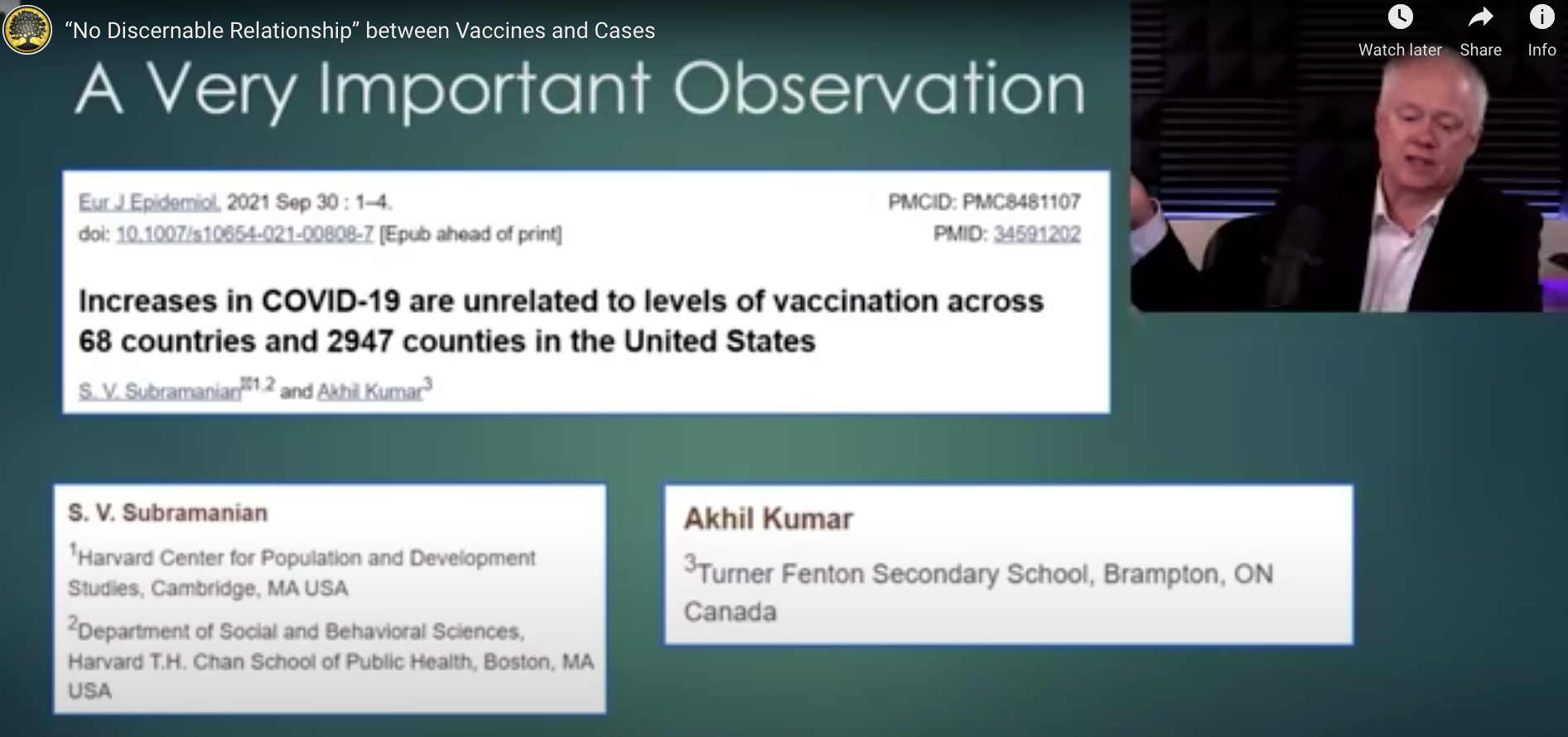
SCREEN SHOT FROM PEAK PROSPERITY VIDEO BELOW.
STORY AT-A-GLANCE
The COVID shots reprogram your immune system to respond in a dysfunctional manner. Aside from increasing vulnerability to infections, this can also result in autoimmune diseases and cancer
A paper published in early May 2021 reported the Pfizer/BioNTech COVID jab “reprograms both adaptive and innate immune responses,” causing immune depletion
Antigens in vaccines have been shown to induce defects in the immune system that can raise the risk of autoimmune diseases
Leaky or nonsterilizing vaccines can also trigger the evolution of more hazardous viruses, and the COVID jabs are among the leakiest “vaccines” ever created
According to health authorities, the vaccine-evading Omicron variant necessitates a third COVID injection, but this recommendation will only perpetuate mutation
From [MERCOLA] A number of medical experts, scientists and published studies now warn that the COVID shots reprogram your immune system to respond in a dysfunctional manner. Aside from increasing vulnerability to infections, this can also result in autoimmune diseases and cancer.
Pfizer Shot Reprograms Both Arms of Your Immune System
A paper1 posted May 6, 2021, on the preprint server medRxiv reported that the Pfizer/BioNTech COVID jab "reprograms both adaptive and innate immune responses," causing immune depletion.
While they confirmed the jab "induced effective humoral and cellular immunity against several SARS-CoV-2 variants," the shot "also modulated the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and nonspecific (viral, fungal and bacterial) stimuli."
In other words, we're looking at a horrible tradeoff. You may get some protection against SARS-CoV-2 and its variants, but you're weakening your overall immune function, which opens the door wide to all sorts of other health problems, from bacterial, fungal and viral infections to cancer and autoimmunity.
After the injection, innate immune cells had a markedly decreased response to toll-like receptors 4, 7 and 8 (TLR4, TLR7, TLR8) ligands, while cytokine responses induced by fungi were stronger. According to the authors, defects in TLR7 have previously been linked to an increased susceptibility to COVID-19 in young males.
People who were "fully vaccinated," having received two doses of the Pfizer shot, also produced significantly less interferon upon stimulation, and this can hamper the initial innate immune response against the virus.
Repeated Vaccinations and the Risk of Autoimmunity
Pathogenic infections and cancer are but two potential outcomes of this kind of reprogramming. Previous research, for example, has linked defects in the immune system to a higher risk of autoimmune diseases. What's more, it's been shown that antigens in vaccines, specifically, can induce this kind of immune system dysfunction.2 As reported in the paper in question:3
"Repeated immunization with antigen causes systemic autoimmunity in mice otherwise not prone to spontaneous autoimmune diseases. Overstimulation of CD4+ T cells led to the development of autoantibody-inducing CD4+ T (aiCD4+ T) cell which had undergone T cell receptor (TCR) revision and was capable of inducing autoantibodies.
The aiCD4+ T cell was induced by de novo TCR revision but not by cross-reaction, and subsequently overstimulated CD8+ T cells, driving them to become antigen-specific cytotoxic T lymphocytes (CTL).
These CTLs could be further matured by antigen cross-presentation, after which they caused autoimmune tissue injury akin to systemic lupus erythematosus (SLE). Systemic autoimmunity appears to be the inevitable consequence of over-stimulating the host's immune 'system' by repeated immunization with antigen, to the levels that surpass system's self-organized criticality."
Fast-forward to mid-May 2021, when a study4 in the Journal of Clinical Investigations reported that "SARS-CoV-2 mRNA vaccines induce broad CD4+ T cell responses that recognize SARS-CoV-2 variants and HCoV-NL63." HCoV-NL63 is a human coronavirus associated with the common cold.
"Interestingly, we observed a 3-fold increase in the CD4+ T cell responses to HCoV-NL63 spike peptides after vaccination," the authors stated, adding, "Our results suggest that T cell responses elicited or enhanced by SARS-CoV-2 mRNA vaccines may be able to control SARS-CoV-2 variants and lead to cross-protection against some endemic coronaviruses."
What they did not address was that excessive CD4a+ T cell responses could also result in the development of autoantibodies and autoimmune disease.
COVID Shots May Also Cause More Hazardous Variants
We've long known that leaky or nonsterilizing vaccines can trigger the evolution of more hazardous viruses.5,6,7,8 So far, SARS-CoV-2 variants have mutated into less dangerous versions, which is fortunate, but the risk of the COVID shots creating a "monster" still remains.
In a February 9, 2021, article,9 NPR highlighted this risk, stating that "vaccines could drive the evolution of more COVID-19 mutants." According to NPR science correspondent Richard Harris, "the virus is always mutating. And if one happens to produce a mutation that makes it less vulnerable to the vaccine, that virus could simply multiply in a vaccinated individual."
The Omicron variant appears to have significant resistance against antibodies produced by the original COVID shots, which is why Omicron infection is being primarily reported in those who have received the injections.
In 2018, Quanta Magazine detailed how vaccines drive the evolution of pathogens.10 I've referenced that article on previous occasions, as have many others. In response, the editor of Quanta Magazine added a "disclaimer" dated December 6, 2021, to the article, stating:
"This article from 2018 discusses how leaky vaccines — vaccines that do not reduce viral replication or transmission to others — can drive the pathogens they target to evolve and become more virulent. These concerns do not apply to COVID-19 vaccines, because COVID-19 vaccines significantly reduce coronavirus replication and transmission, reducing the chance that mutations occur and variants arise ..."
That statement is clearly false, as studies have repeatedly shown the COVID shots are in fact leaky. They do not "significantly reduce" viral replication or transmission, as the editor claims. Quite the opposite.
People who have received one or more COVID shots have been found to harbor higher viral loads than the unvaccinated, and Israel (which appears to have the best tracking and monitoring) reports that the worst COVID cases are in those who are fully vaxxed.
December 6, 2021, Newsweek11 reported a COVID outbreak among "fully vaccinated" hospital staff in Spain. After a Christmas dinner with more than 170 fully vaxxed health care workers in attendance, nearly 70 of them tested positive for COVID. Some reported mild symptoms. Daniel Horowitz pointed out the editor's false note in a December 9, 2021, Blaze post:12
"Leaky vaccines are worse than no vaccine at all. That is the unmistakable conclusion one would derive from a May 2018 article in Quanta magazine, a top scientific publication, about the unsuccessful attempts to create vaccines for HIV, malaria, and anthrax that aren't leaky and don't run the risk of making the pathogens more dangerous.
Yet now that we are seeing such a microbiological Frankenstein play out in real life and people like Dr. Robert Malone have been citing this article to raise red flags about the leaky COVID shots, Quanta magazine took the unprecedented step of slapping an editor's note on an article three and a half years later to get people to stop applying it to the leakiest vaccine of all time."
COVID Shots Stop Working Within a Few Months
A study in the New England Journal of Medicine, published December 9, 2021, also confirms that whatever protection you get from the Pfizer COVID shot is short in duration. As explained by the authors:13
"In December 2020, Israel began a mass vaccination campaign against coronavirus disease 2019 (Covid-19) by administering the BNT162b2 vaccine, which led to a sharp curtailing of the outbreak.
After a period with almost no cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, a resurgent Covid-19 outbreak began in mid-June 2021. Possible reasons for the resurgence were reduced vaccine effectiveness against the delta (B.1.617.2) variant and waning immunity.
We used data on confirmed infection and severe disease collected from an Israeli national database for the period of July 11 to 31, 2021, for all Israeli residents who had been fully vaccinated before June 2021.
We used a Poisson regression model to compare rates of confirmed SARS-CoV-2 infection and severe Covid-19 among persons vaccinated during different time periods, with stratification according to age group and with adjustment for possible confounding factors.
Among persons 60 years of age or older, the rate of infection in the July 11-31 period was higher among persons who became fully vaccinated in January 2021 (when they were first eligible) than among those fully vaccinated 2 months later, in March (rate ratio, 1.6 ...)
Among persons 40 to 59 years of age, the rate ratio for infection among those fully vaccinated in February (when they were first eligible), as compared with 2 months later, in April, was 1.7 ... Among persons 16 to 39 years of age, the rate ratio for infection among those fully vaccinated in March (when they were first eligible), as compared with 2 months later, in May, was 1.6 ...
The rate ratio for severe disease among persons fully vaccinated in the month when they were first eligible, as compared with those fully vaccinated in March, was 1.8 ... among persons 60 years of age or older and 2.2 ... among those 40 to 59 years of age ...
These findings indicate that immunity against the delta variant of SARS-CoV-2 waned in all age groups a few months after receipt of the second dose of vaccine."
Two Doses Aren't Enough
Earlier this year, vaccine makers and health authorities said the shots were about 95% effective and if enough people got the shots, normalcy would be restored. We now know that was a false promise. The goal post was moved back with the emergence of Delta and then Omicron, for which we're now told we need a third booster.
December 13, 2021, Reuters14 reported that British scientists have concluded "two-dose COVID-19 vaccine regimens do not induce enough neutralizing antibodies against the Omicron coronavirus variant," and that "increased infections in those previously infected or vaccinated may be likely."
'Just Deal With' Booster Shots, Fauci Says
When in mid-December 2021, Dr. Anthony Fauci was asked if Americans should expect annual COVID boosters, he replied in the affirmative, saying that Americans will "just have to deal with" the prospect of getting boosters at regular intervals.15 So, in essence, Fauci wants us to accept that booster deficiency is the reason why the COVID-19 "pandemic" continues.
Clearly, that is not the case. The real reason COVID is still an issue is because Fauci and the medical establishment have suppressed viable early treatments. If early treatment was the norm, COVID would rapidly become a distant memory.
As predicted over a year ago, we're now on an injection treadmill with no end in sight, and every single dose carries the risk of serious side effects, up to and including permanent disability and death. The only scientifically sound way out of this failed experiment is to stop. No more boosters.
Instead, the captured U.S. Food and Drug Administration granted emergency use authorization to novel gene transfer technologies that don't work like conventional vaccines in that they don't prevent infection and spread, thus creating an evil cycle of new vaccine-resistant variants. As demonstrated by James Lyons-Weiler (in a now broken weblink), the more we vaccinate, the higher the COVID caseload.

Weiler's graph looks very much like that in a September 30, 2021, study16 in the European Journal of Epidemiology, which found that the higher the vaccination rate in a given area, the higher the COVID case rate.
Dr. Chris Martenson discusses this finding in the video below. As noted by Martenson, "the line goes the wrong way," meaning the more heavily "vaccinated" a population is, the worse things get.
As predicted over a year ago, we're now on an injection treadmill with no end in sight, and every single dose carries the risk of serious side effects, up to and including permanent disability and death. The only scientifically sound way out of this failed experiment is to stop. No more boosters.
Fortunately, it seems most Americans are starting to catch on, and so far, the fearmongering around Omicron has not resulted in a rush for boosters.17 According to an Axios/Ipsos poll conducted December 10 through December 13, 2021, 67% of unvaccinated respondents said Omicron makes no difference in their decision of whether to get vaccinated; 19% said it makes them more likely while 11% said it makes them less likely to get the shot.
Among respondents who already had received one or two doses, 59% said Omicron makes no difference in their decision to get a third dose; 36% said it makes them more likely and 5% said it makes them less likely to get it.
Considering the shots have been shown to deregulate your immune function, it would be wise to "just say no" to further boosters. Should you develop symptoms of SARS-CoV-2 infection, remember there are safe and effective early treatment protocols, including the I-MASK+18 and I-MATH+,19 protocols, which are available for download on the COVID Critical Care website in multiple languages. Other protocols that have great success are:
Tess Laurie's World Council for Health protocol
This is a load of information to review, especially if you are fatigued and sick with COVID or have a family member struggling. After reviewing all of these protocols, I believe the Front Line COVID-19 Critical Care Alliance's protocol is among the easiest to follow. Below is a summary of that protocol, with minor amendments.
Sources and References
Juvenile Jail Cops in KS Shackled a Handcuffed Black Teen’s Ankles and then Held Him Prone, Assaulted and Killed Him. Arrested for Refusal to Consent to Detention after Foster Fam Called Cops for Eval
/
From [HERE] A 17-year-old Black boy who died in police custody after being restrained at a juvenile jail in Kansas died by homicide, according to a Sedgwick County autopsy report.
Cedric Lofton, a Black teenager, was taken into custody on Sept. 24 after his foster father called 911 to say his son was having a mental breakdown and needed an evaluation.
When Lofton refused to go voluntarily, he was arrested for battering a law enforcement officer and taken, restrained, to the Sedgwick County juvenile detention facility.
After staff members decided he was too uncooperative after he allegedly punched an employee, Lofton was shackled at the ankles, rolled into a prone position and handcuffed behind his back, according to the autopsy, released Monday.
Minutes after he was handcuffed, Lofton no longer had a pulse and staff began chest compressions.
He died two days later.

The coroner ruled his death from “complications of cardiopulmonary arrest sustained after physical struggle while restrained in the prone position” and labeled it a homicide.
“As supported by the video evidence, these individuals unjustifiably and with excessive and unreasonable force pinned Cedric to the ground, ultimately killing the unarmed, 135-pound, 17-year-old African American teenager,” a lawyer for Lofton’s family said in a statement to the Daily News Tuesday.
“Cedric’s family anxiously awaits the findings of the criminal investigation and believes the Sedgwick County District Attorney should pursue criminal charges against the law enforcement personnel responsible for Cedric’s death. Cedric’s death was caused by the hands of the very authorities that were obligated to protect him and make sure he was safe. Instead, they killed him with conscious disregard for the young life in their keeping.”
Sedgwick County District Attorney Marc Bennett told The News Tuesday that his office is “in the process of reviewing the autopsy completed by the Sedgwick County Regional Forensic Science Center as well as the lengthy investigation conducted by agents with the Kansas Bureau of Investigations and investigators with the Sedgwick County Sheriff’s Department.”
On COVID Injections: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination - Sucharit Bhakdi, MD and Arne Burkhardt, MD
/Sucharit Bhakdi, MD and Arne Burkhardt, MD
From {HERE] and [PDF] This text is a written summary of Dr. Bhakdi’s and Dr. Burkhardt’s presentations at the Doctors for COVID Ethics symposium that was live-streamed by UKColumn on December 10th, 2021. The two presentations can be viewed at the very beginning of the video recording of the symposium.
The authors
Dr. Bhakdi has spent his life practicing, teaching and researching medical microbiology and infectious diseases. He chaired the Institute of Medical Microbiology and Hygiene at the Johannes Gutenberg Unversity of Mainz, Germany, from 1990 until his retirement in 2012. He has published over 300 research articles in the fields of immunology, bacteriology, virology and parasitology, and served from 1990 to 2012 as Editor-in-Chief of Medical Microbiology and Immunology, one of the first scientific journals of this field that was founded by Robert Koch in 1887.
Dr. Arne Burkhardt is a pathologist who has taught at the Universities of Hamburg, Berne and Tübingen. He was invited for visiting professorships/study visits in Japan (Nihon University), the United States (Brookhaven National Institute), Korea, Sweden, Malaysia and Turkey. He headed the Institute of Pathology in Reutlingen for 18 years. Subsquently, he worked as an independent practicing pathologist with consulting contracts with laboratories in the US. Burkhardt has published more than 150 scientific articles in German and international scientific journals as well as contributions to handbooks in German, English and Japanese. Over many years he has audited and certified institutes of pathology in Germany.
The evidence
We herewith present scientific evidence that calls for an immediate stop of the use of gene-based COVID-19 vaccines. We first lay out why the agents cannot protect against viral infection. While no positive effects can be expected, we show that the vaccines can trigger self-destructive processes that lead to debilitating illness and death.
Why the vaccines cannot protect against infection
A fundamental mistake underlying the development of the COVID-19 vaccines was to neglect the functional distinction between the two major categories of antibodies which the body produces in order to protect itself from pathogenic microbes.
The first category (secretory IgA) is produced by immune cells (lymphocytes) which are located directly underneath the mucous membranes that line the respiratory and intestinal tract. The antibodies produced by these lymphocytes are secreted through and to the surface of the mucous membranes. These antibodies are thus on site to meet air-borne viruses, and they may be able to prevent viral binding and infection of the cells.
The second category of antibodies (IgG and circulating IgA) occur in the bloodstream. These antibodies protect the internal organs of the body from infectious agents that try to spread via the bloodstream.
Vaccines that are injected into the muscle – i.e., the interior of the body – will only induce IgG and circulating IgA, not secretory IgA. Such antibodies cannot and will not effectively protect the mucous membranes from infection by SARS-CoV-2. Thus, the currently observed “breakthrough infections” among vaccinated individuals merely confirm the fundamental design flaws of the vaccines. Measurements of antibodies in the blood can never yield any information on the true status of immunity against infection of the respiratory tract.
The inability of vaccine-induced antibodies to prevent coronavirus infections has been reported in recent scientific publications.

The vaccines can trigger self-destruction
A natural infection with SARS-CoV-2 (coronavirus) will in most individuals remain localized to the respiratory tract. In contrast, the vaccines cause cells deep inside our body to express the viral spike protein, which they were never meant to do by nature. Any cell which expresses this foreign antigen will come under attack by the immune system, which will involve both IgG antibodies and cytotoxic T-lymphocytes. This may occur in any organ. We are seeing now that the heart is affected in many young people, leading to myocarditis or even sudden cardiac arrest and death. How and why such tragedies might causally be linked to vaccination has remained a matter of conjecture because scientific evidence has been lacking. This situation has now been rectified.
Histopathologic studies: the patients
Histopathologic analyses have been performed on the organs of 15 persons who died after vaccination. The age, gender, vaccination record, and time of death after injection of each patient are listed in the table on the next page. The following points are of utmost importance:
Prior to death, only 4 of the 15 patients had been treated in the ICU for more than 2 days. The majority were never hospitalized and died at home (5), on the street (1), at work (1), in the car (1), or in home-care facilities (1). Therefore, in most cases, therapeutic intervention is unlikely to have significantly influenced the post-mortem findings.
Not a single death was brought into any possible association with the vaccination by the coroner or the public prosecutor; this association was only established by our autopsy findings.
The initially performed conventional post-mortems also uncovered no obvious hints to a possible role of vaccination, since the macroscopic appearance of the organs was overall unremarkable. In most cases, “rhythmogenic heart failure” was postulated as the cause of death.
But our subsequent histopathological analyses then brought about a complete turnaround. A summary of the fundamental findings follows.


Dr. Thomas Binder: 'The alleged pandemic is mainly an unreal PCR testing pandemic, but the totalitarian measures it has spawned are real: they threaten our freedom, our livelihoods and even our lives'
/
From [HERE] and [HERE] Dr. Thomas Binder, a Swiss cardiologist and member of D4CE, has written a strong and accessible piece debunking the prevailing corona narrative for the general public.
Thomas’ article is available in full from his website.
Thomas has documented three events which presaged the current corona fake pandemic:
The conjuring up, in 2006, of a fictitious epidemic of whooping cough, based on nothing more than PCR Testing: “Faith in Quick Test Leads to Epidemic That Wasn’t”.
The Swine Flu Scandal, 2009: “Profiteers of Fear – The Swine Flu Racket” (German).
“Event 201:” Corona Pandemic Simulation, 2019. See the movie “Event 201: Corona Pandemic from the Drafting Table,” produced in German with English subtitles
Thomas also counters the “top 10” myths about the prevailing corona narrative with the following arguments:
There is no epidemic of COVID-19 in any country – in most countries, there has been no excess mortality.
It is wrong to test symptomatic people for only one of all respiratory viruses, and it is even more wrong to test asymptomatic people.
The Corman-Drosten PCR protocol, which was hastily developed and prematurely adopted by the WHO, is technically flawed and not fit for the purpose of diagnosing an infection with the virus.
Asymptomatic transmission of respiratory viruses is not epidemiologically relevant.
Effective prevention measures and treatments for COVID-19 do exist.
SARS-CoV-2 mutate slowly but inexorably. Therefore, even the most effective vaccines will always lag behind the new variants.
SARS-CoV-2 is becoming more and more contagious indeed, but less and less dangerous, following the laws of evolution.
SARS-CoV-2 does not occur perennially but seasonally from late fall to early spring.
The basic and cross-immunity protect 80-90% of the population from contracting the seasonal beta corona and influenza viruses, which also applies to SARS-CoV-2.
It is not possible to stop the alleged pandemic of the alleged killer virus through vaccination, since the vaccines, aside from causing grave disease, have also proven ineffective.
At the end of the article, Thomas supports his conclusions using real-time ICU occupancy data from Zurich ETH, as shown in the featured picture. The near-real-time monitoring of intensive care occupancy by ETH Zurich, dated November 26th, 2021, exposes the fundamental fraudulence of the prevailing corona narrative. The graph shows that each of the alleged spikes of COVID-19 cases is always mirrored by a decline in non-COVID cases, indicating misdiagnosis of other respiratory infections as COVID.