So-Called New COVID “Variant" was Simulated in Israel Weeks before it was “Discovered" [“in reality there are no variants of COVID. They are all computer simulations of specific gene sequences"]
/
the editor of Health Impact News states, “The flames of “COVID fear” are being stoked again, as the Big Pharma Globalists unleash their new plan to increase profits and exert more tyrannical control over populations by using their corporate media and puppet politicians in an attempt to extend the false “COVID pandemic.”
Within just a couple of days after announcing that a “new variant” has been discovered in Africa, Big Pharma has now promised the world that they are rushing to rescue everyone with new drugs and new vaccines to fight this “deadly new variant.”
What kind of people are still watching this Hollywood-like scripted show and actually believing it is true?? [MORE]
From [HERE] Two weeks before this current new variant suddenly appeared in Africa and started making the news cycle, Israel, which has been Pfizer’s human laboratory to test their COVID shots, ran a “war games” simulation to prepare for a “deadly new variant” which at the time had not yet been named. They called this future variant “Omega,” and the simulation was carried out on November 11, 2021.
Dozens of top officials took part in what Prime Minister Naftali Bennett called a COVID-19 war exercise on Thursday to gauge the country’s preparedness for the next wave of the pandemic.
“We are starting an unprecedented event here,” the prime minister said at the start of the exercise – “not only on an Israeli scale but on a global level. We are conducting a war exercise to prepare for a new variant that does not even exist yet.”
The “Omega Exercise,” as Bennett called it, was held in the format of a “war game,” the Prime Minister’s Office said. Bennett has regularly referred to the “Omega strain,” the next harmful COVID-19 variant that has not yet been discovered. A war game is a game of the mind; no physical exercises took place.
Bennett said that Israel has surfaced from the Delta wave without locking down, proving that “with proper management, the pandemic can be defeated.” (Full article – and thanks to the Robin Monotti, Dr Mike Yeadon & Cory Morningstar Telegram Channel for pointing this out.)
Africa is Chosen to be the Source of the New Variant Scam
Up until now, Africa has been an enigma to the Globalists’ narrative on the COVID-19 plandemic, as the continent has the lowest rates of COVID-19 vaccination, while also having the fewest amounts of “COVID-19 deaths.”
Ryan McMaken of the Mises Institute reported:
Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Then, once vaccines became available, the narrative was modified to “Get shots in arms and then covid will stop spreading. Those countries without vaccines, on the other hand, will continue to face mass casualties.”
The lockdown narrative, of course, has already been thoroughly overturned. Jurisdictions that did not lock down or adopted only weak and short lockdowns ended up with covid death tolls that were either similar to—or even better than—death tolls in countries that adopted draconian lockdowns. Lockdown advocates said locked-down countries would be overwhelmingly better off. These people were clearly wrong.
Undaunted by the increasing implausibility of the lockdown narrative, the global health bureaucrats are nonetheless doubling down on forced vaccines—as we now see in Austria—and we continue to be assured that only countries with high vaccination rates can hope to avoid disastrous covid outcomes.
Yet, the experience in sub-Saharan Africa calls both these narratives into question: Africa’s numbers have been far, far lower than the experts warned would be the case.
For example, the AP reported this week that in spite of low vaccination rates, Africa has fared better than most of the world:
[T]here is something “mysterious” going on in Africa that is puzzling scientists, said Wafaa El-Sadr, chair of global health at Columbia University. “Africa doesn’t have the vaccines and the resources to fight COVID-19 that they have in Europe and the U.S., but somehow they seem to be doing better,” she said….
Fewer than 6% of people in Africa are vaccinated. For months, the WHO has described Africa as “one of the least affected regions in the world” in its weekly pandemic reports.
Yet disaster for Africa has long been predicted for several reasons even beyond the availability of vaccines. For instance, it is known that lockdowns are especially impractical in the poorest parts of the world.
This is because populations in places with undeveloped economies can’t simply sit at home and live off savings or debt. Rather, these people must go out into the world and earn a living on a day-to-day basis. Starvation is the alternative.
Moreover, much of this work is done in the informal economy, so enforcing lockdowns becomes especially difficult.
It was also assumed covid would be especially deadly in Africa due to the fact many large households live in small housing units.
But that “conventional wisdom” flies in the face of the reality of covid in Africa, which is that there have been fewer deaths. (Full article here.)
But this new fake variant has been reportedly found in South Africa, with the supposed first detections coming from Botswana. The variant now has a name, Omicron, and while the corporate media is hyping it up and creating fear over it, the people in Africa themselves are not concerned.
Paul Joseph Watson of Summit News reports:
The new ‘Omicron’ variant of COVID-19 was first detected in four people who were fully vaccinated, according to a public statement by the Botswana government.
The new variant, which some claim is three times more contagious, was initially discovered in Botswana before it spread across South Africa.
The news was met with global alarm, prompting financial markets to plummet and new travel bans to be put in place.
According to a public statement by the Botswana government, the new mutation was first discovered in four people who had received both doses of the COVID-19 vaccine.
Covid Still Has No Clearly Defined Symptoms b/c It is Determined by PCR Tests. Study Concludes common cold and gastrointestinal symptoms are wrongly associated with Covid
/
From [HERE] A diagnosis is a compilation of clinical symptoms and testing adds further information to help doctors decide on the likelihood of a particular diagnosis. Because a covid case has been defined not by symptoms but by a positive test result this logic has been reversed. The consequence of this was an ever growing list of symptoms associated with the disease and even the concept of an ‘asymptomatic case’.
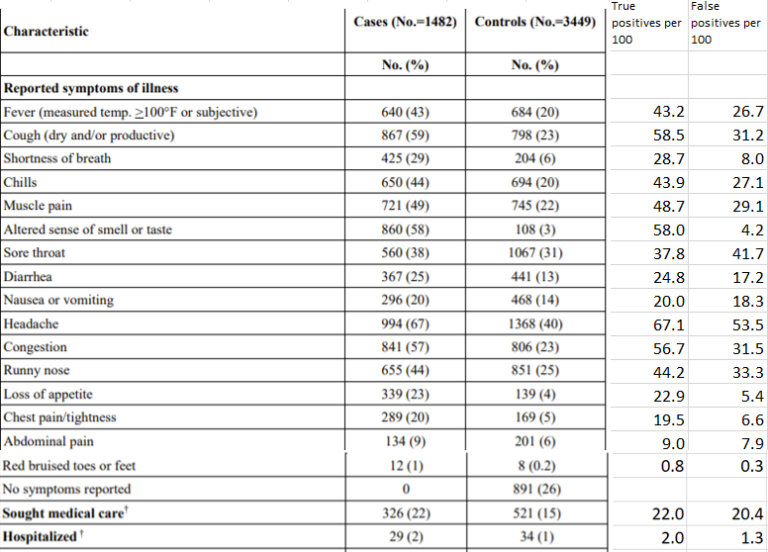
After 20 months of covid it is quite incredible that the symptoms associated with the disease have not been clearly defined. It is possible to figure out which symptoms are associated with a positive test and that has incidentally been reported in a paper in the New England Journal of Medicine studying vaccine efficacy among healthcare workers in the first five months of 2021. Using data from this paper symptoms such as sore throat, runny nose, diarrhoea, nausea, vomiting and abdominal pain can be shown to have no bearing on whether someone will test positive for covid.
The study measured healthcare workers who were tested to see if they had covid, and were asked about vaccination status but also which symptoms they had before testing. The paper then reported the proportion testing positive or negative. For example, they report that 9% of people with abdominal pain tested positive compared to 6% testing negative. Therefore, it might be assumed that abdominal pain is a relevant symptom for covid. However, the authors had included asymptomatic people among the negative control group and not the positives. This meant that the denominator for the percentage was too high in the negative group. Excluding the asymptomatic people from both groups gives a true percentage for comparison.

Figure 2 Sensitivity of each symptom as a test (percentage of people with the disease who have that symptom) and specificity of each symptom as a test (percentage of people without the disease who do not have that symptom)
To really understand the implications of each symptom we can treat each one as if whether or not you have it is, itself, a test for covid. In this way, we can calculate the percentage of people with the disease who have that symptom, the sensitivity of the symptom as a test. Likewise we can calculate the chance of someone testing negative if they do not have that symptom, the specificity of the symptom as a test. The latter gives an indication of the types of symptoms that people use to make the decision to seek a test.
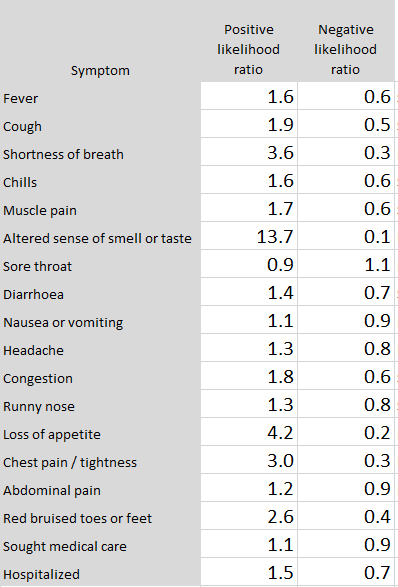
Having broken down the problem this way it is possible to calculate a practical indicator of the meaning of each symptom. The first stage is to calculate the likelihood ratios. This is an intermediate step that leads us to the probability of someone with each symptom testing positive. [MORE]
Analysis Suggests the English Government May be Manipulating Mortality Data to Fabricate the Effectiveness of Deadly COVID Injections
/Latest statistics on England mortality data suggest systematic miscategorisation of vaccine status and uncertain effectiveness of Covid-19 vaccination
By Martin Neil, Norman Fenton Joel Smalley, Clare Craig, Joshua Guetzkow, Scott McLachlan, Jonathan Engler and Jessica Rose
3 December 2021
From [HERE] and [HERE] The risk/benefit of Covid vaccines is arguably most accurately measured by an all-cause mortality rate comparison of vaccinated against unvaccinated, since it not only avoids most confounders relating to case definition but also fulfils the WHO/CDC definition of "vaccine effectiveness" for mortality. We examine the latest UK ONS vaccine mortality surveillance report which provides the necessary information to monitor this crucial comparison over time. At first glance the ONS data suggest that, in each of the older age groups, all-cause mortality is lower in the vaccinated than the unvaccinated. Despite this apparent evidence to support vaccine effectiveness-at least for the older age groups-on closer inspection of this data, this conclusion is cast into doubt because of a range of fundamental inconsistencies and anomalies in the data. Whatever the explanations for the observed data, it is clear that it is both unreliable and misleading. While socio-demographical and behavioural differences between vaccinated and unvaccinated have been proposed as possible explanations, there is no evidence to support any of these. By Occam's razor we believe the most likely explanations are systemic miscategorisation of deaths between the different categories of unvaccinated and vaccinated; delayed or non-reporting of vaccinations; systemic underestimation of the proportion of unvaccinated; and/or incorrect population selection for Covid deaths.
Our recent articles [1, 2] have argued that the simplest and most objective way to assess the overall risk/benefit of Covid-19 vaccines is to compare all-cause mortality rates of the unvaccinated against the vaccinated in each separate age-group. For such an assessment we need accurate periodic data on both age-categorized deaths and the number of vaccinated/unvaccinated people in each age group for that period.
Any systemic errors or biases can lead to conclusions that are inversions of the real situation. For example, simply reporting deaths one week late when a vaccine programme is rolled out will (with statistical certainty) lead to any vaccine, even a placebo, seemingly reducing mortality. The same statistical illusion will happen if any death of a person occurring in the same week as the person is vaccinated is treated as an unvaccinated, rather than vaccinated, death [16].
The UK Government (through its various relevant agencies) has been better than most countries in providing detailed data on Covid cases and deaths indexed by vaccine status. However, in [1] we highlighted the absence of relevant age-categorized mortality data for England, and major inconsistencies in the data provided by different agencies. Of most concern are the very different estimates provided by UKHSA (United Kingdom Health Security Agency) and the ONS (Office for National Statistics) of the number of vaccinated and unvaccinated people. The reports from UKHSA use estimates from the NIMS (National Immunisation Management Service) database [10], while the estimates from the ONS are based on 2011 census respondents and patients registered with a GP in 2019. Hence the ONS England ‘population’ (which therefore includes only people aged at least 10) is only approximately 39 million, compared to the approximately 49 million listed in NIMS. While our focus is on mortality by vaccination status, accurate periodic estimates for the proportion of people vaccinated are also crucial for determining vaccine effectiveness, since this is simply a comparison between the ‘cases’, hospitalisations and deaths per 100K vaccinated and unvaccinated.
An indication of just how critical this is illustrated by the latest UKHSA report [3] which showed that, in each age group above 29, the Covid case rate was higher among the vaccinated than the unvaccinated.
The FDA Now Wants the Public to Wait Until 2096 to Disclose All Information it Relied On to Approve Pfizer’s COVID Injection. The Govt Doubles Down in its 2nd Request to Court to Delay FOIA Response
/
From [AARONSIRI,ESQ] A prior post explained that the FDA has asked a federal judge to make the public wait until the year 2076 to disclose all of the data and information it relied upon to license Pfizer’s COVID-19 vaccine. Literally, a 55-year delay. My firm, on behalf of PHMPT, asked that this information be disclosed in 108 days – the same amount of time it took for the FDA to review and license Pfizer’s vaccine.
The Court ordered the parties to submit briefs in support of their respective positions by December 6, 2021. The FDA’s brief, incredibly, doubles down. It now effectively asks to have until at least 2096 to produce the Pfizer documents. Not a typo. A total of at least 75 years.
Other than producing an initial ~12,000 pages in around two months, the FDA thereafter only wants to commit to producing 500 pages per month. The FDA also disclosed that it actually has approximately at least 451,000 pages to produce.*
Each side gets to file response briefs on December 13, 2021, and then there is oral argument on December 14, 2021 before the Judge. If you want to read the response to the FDA’s position, a copy of the introduction in the brief my firm filed is below. And below that, a downloadable copy of each side’s full briefing is available.
Enjoy. And if you find what you are reading difficult to believe – that is because it is dystopian for the government to give Pfizer billions, mandate Americans to take its product, prohibit Americans from suing for harms, but yet refuse to let Americans see the data underlying its licensure. The lesson yet again is that civil and individual rights should never be contingent upon a medical procedure.
EXCERPT FROM BRIEF DEMANDING TIMELY PRODUCTION
INTRODUCTION
A minimum of 20,010 days (54 years and 10 months). That is how long the FDA proposes to take, at a rate of 500 pages per month, to produce only a portion of the documents in its file for the COVID-19 Pfizer vaccine that PHMPT requested pursuant to the Freedom of Information Act (the “FOIA Request”) and 21 C.F.R. § 601.51(e). But when it came to reviewing those same documents to license this product so that Pfizer could freely sell it to the public, the FDA took just 108 days. It took the FDA’s parent department even less time to grant Pfizer complete immunity to liability for injuries from this product, and it took a stroke of the President’s pen to mandate this product for federal employees, the private sector and military personnel.
The federal government mandating that millions of people be injected with a liability-free vaccine requires complete government transparency – not the government’s suppression of information. PHMPT is comprised of independent scientists working at some of our nation’s premier institutions, and all they are seeking is the data the FDA has already reviewed concerning the Pfizer vaccine in order to provide the necessary peer review. The FDA knows that they, and other independent scientists, cannot properly analyze that data until it is all released. Yet, the FDA wants to wait until most of those scientists are long since dead to fully release the data. News outlets, politicians, and scientists have called the FDA’s position “outrageous.” They are correct.
The entire purpose of FOIA is government transparency. In multiple recent cases, in upholding the FOIA’s requirement to “make the records promptly available,” courts have required agencies, including the FDA, to produce 10,000 or more pages per month, and those cases did not involve a request nearly this important – i.e., the data underlying licensure of a liability-free product that the federal government requires nearly all Americans to receive. As the present pandemic rages on, independent review of these documents by outside scientists is urgently needed to assist with addressing the shortcomings and issues with the response to the pandemic to date. [MORE]
COVID Injections Have Created 9 Billionaires So Far. Would Profiteers Still be Making Billions If They Could Be Held Liable for the Injuries and Death Caused by their Vax Injections?
/
WOULD YOU EAT HERE? HOW MANY HAVE DIED OR BEEN INJURED OR WILL DIE OR BECOME DISEASED DUE TO COVID INJECTIONS? THE SCIENCE FREE MEDICINE PARROTED BY THE DEPENDENT MEDIA IS KILLING PEOPLE.
From [HERE] The federal government has given complete immunity to Pfizer, Moderna, and J&J for any injury caused by their Covid-19 vaccines. That’s right: you cannot sue them if you are injured by their Covid-19 vaccine. (See Note 1 to read the law yourself.) So, while their product may not give you immunity, they are guaranteed immunity.
And it gets even worse. These companies are even immune for – hold your breath – willful misconduct. That may sound crazy, but it is shockingly true. You can only sue them for willful misconduct if the federal government first sues them for such conduct. (See Note 2 to read the law yourself.) And what are the odds the federal government will do so after wildly promoting the vaccine? About as likely as the FDA ever admitting they promoted a vaccine that caused widespread harm.
So, despite Pfizer’s history of willful misconduct, and that this is Moderna’s first product, and that they going to rake in over $100 billion selling a product millions of Americans are mandated to take, you cannot sue them for injuries. That seems fair. After all, we should take pity on these companies since this revenue may not be sufficient to pay for the injuries.
What is most incredible is that we are talking about a product that does not prevent infection and transmission. It, at best, provides personal protection. So, you cannot say “no” to the product without losing your job, cannot sue if you are injured, cannot see the data underlying its licensure, all while it can only potentially protect … you! What?!
From [HERE] At least nine people have become new billionaires since the beginning of the COVID pandemic, thanks to the excessive profits pharmaceutical corporations with monopolies on COVID vaccines are making. Vaccine billionaires are being created as stocks in pharmaceutical firms rise rapidly in expectation of huge profits from the COVID-19 vaccines over which these firms have monopoly control.
The 9 new vaccine billionaires, in order of their net worth are:
Stéphane Bancel, Moderna’s CEO (worth $4.3 billion)
Ugur Sahin, CEO and co-founder of BioNTech (worth $4 billion)
Timothy Springer, an immunologist and founding investor of Moderna (worth $2.2bn)
Noubar Afeyan, Moderna’s Chairman (worth $1.9 billion)
Juan Lopez-Belmonte, Chairman of ROVI, a company with a deal to manufacture and package the Moderna vaccine (worth $1.8 billion)
Robert Langer, a scientist and founding investor in Moderna (worth $1.6 billion)
Zhu Tao, co-founder and chief scientific officer at CanSino Biologics (worth $1.3 billion)
Qiu Dongxu, co-founder and senior vice president at CanSino Biologics (worth $1.2)
Mao Huihua, also co-founder and senior vice president at CanSino Biologics (worth $1 billion)
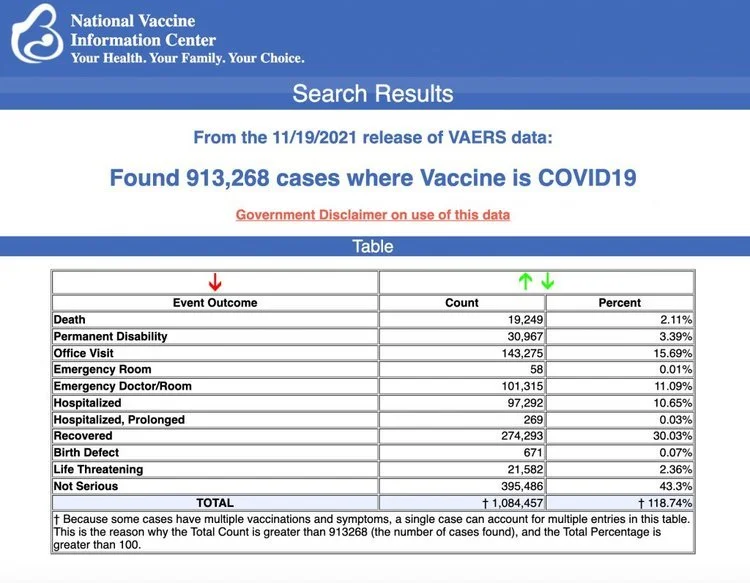
The Centers for Disease Control and Prevention released new data last Monday showing a total of 913,268 adverse events following COVID vaccines were reported between Dec. 14, 2020, and Nov. 19, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 19,249 reports of deaths — an increase of 396 over the previous week — and 143,395 reports of serious injuries, including deaths, during the same time period — up 4,269 compared with the previous week.
Dr. David Martin Exposes The COVID Profiteers
8 Top Pfizer, Moderna Shareholders $10 Billion Richer After Dependent Media Hypes Omicron Fears
/From [CHD} In the week after news of the Omicron variant hit the headlines, the CEOs and major shareholders of Moderna and Pfizer made a combined $10.31 billion, according to data compiled by the UK-based Global Justice Now.
Shares of Moderna jumped 13.61% — $273.39 to $310.61 — between Nov. 24 and Dec. 1, while Pfizer shares increased 7.41% — $50.91 to $54.68, Common Dreams reported.
Moderna CEO Stéphane Bancel saw his shares increase from $6.1 billion to $6.9 billion, for a gain of $824 million. Albert Bourla, CEO of Pfizer, saw gains of $339,291.
Combined with the CEOs, Moderna’s and Pfizer’s four top shareholders made about $5.16, The Daily Mail reported.
The top Pfizer shareholders include Vanguard Group ($1.72 billion), Blackrock ($1.46 billion), State Street Corp. ($1.1 billion) and Capital World Investors ($909 million).
Moderna’s top shareholders are Baillie Gifford & Co. ($1.59 billion), Vanguard Group ($1 billion), Blackrock ($999.1 million) and Flagship Pioneering ($653.7 million).
As The Defender reported Nov. 30, early news reports on Omicron sent vaccine makers’ stocks soaring, after Moderna and Pfizer said they were rushing to develop vaccines for the new variant.
Moderna’s stock rose 20% on the Friday following Thanksgiving — a short trading day — while Pfizer and its vaccine partner BioNTech saw respective gains of 6% and 14%.
No evidence we need a vaccine for Omicron, but Pfizer makes the case, anyway
Global Justice Now accused Big Pharma of being responsible for the emergence of Omicron by gobbling up profits selling vaccines to wealthy countries, while refusing to share patents and making sure low-income countries get access to COVID vaccines.
Tim Bierley, the organization’s pharma campaigner, said:
“Pharmaceutical companies knew that grotesque levels of vaccine inequality would create prime conditions for new variants to emerge. They let COVID-19 spread unabated in low and middle-income countries. And now the same pharma execs and shareholders are making a killing from a crisis they helped to create. It’s utterly obscene.”
But not everyone agrees that failure to vaccinate causes new variants to emerge, or that Omicron is dangerous.
Dr. Angelique Coetzee, who is credited with discovering the Omicron variant, said she believes the variant may help lead to herd immunity.
Coetzee, who chairs the South African Medical Association and who has been a general practitioner for the last 33 years, said Omicron symptoms so far appear mild.
Coetzee wrote for The Daily Mail:
“No one here in South Africa is known to have been hospitalized with the Omicron variant, nor is anyone here believed to have fallen seriously ill with it … The simple truth is: We don’t know yet anywhere near enough about Omicron to make such judgments or to impose such policies … If, as some evidence suggests, Omicron turns out to be a fast-spreading virus with mostly mild symptoms for the majority of the people who catch it, that would be a useful step on the road to herd immunity.”
Early data support Coetzee’s observation that while Omicron may be highly infectious, it’s not highly dangerous.
According to CNBC, the South African Medical Research Council, in a report released Saturday, said most patients admitted to a hospital in Pretoria who had COVID didn’t need supplemental oxygen.
The report also noted that many patients were admitted for other medical reasons and were then found to have COVID.Pfizer CEO Bourla responded to that news by telling the Wall Street Journal:
“I don’t think it’s good news to have something that spreads fast. Spreads fast means it will be in billions of people and another mutation may come. You don’t want that.”
Though it’s not clear whether there’s a need for a new shot, Pfizer can develop a vaccine that targets omicron by March 2022, Bourla said.
It will take a few weeks to determine whether the current vaccines provide enough protection against the variant, Bourla said.
3 Teens Dead, 120 Hospitalized in Vietnam Following Pfizer Vax Rollout. No One Can be Held Liable. Dependent Media Ignores Story to Avoid a Conflict of Interest w/Vested Interests who Pay Their Bills
/
From [CHD] The Vietnamese province of Thanh Hoa suspended a batch of Pfizer-BioNTech’s COVID vaccineafter more than 120 teens were hospitalized after being vaccinated.
According to the province’s Center for Disease Control (CDC), the teens were hospitalized for symptoms ranging from nausea and high fevers to breathing difficulties — with 17 children exhibiting severe reactions.
Thanh Hoa authorities have yet to confirm Pfizer’s COVID vaccine caused the teens’ symptoms, VN Express International reported.
Vu Van Chinh, director of the Ha Trung District General Hospital, said side-effects following vaccination are normal but are more likely to happen in children than adults.
Luong Ngoc Truong, director of the CDC, said although the province stopped using the current vaccine batch, “We still have other batches, also Pfizer vaccines, so we will continue vaccinating the children.”
The suspended batch was put into storage and could be used later for other groups like adults, Truong added.
Last week, four workers in Thanh Hoa’s Kim Viet Shoe factory died — also due to “overreaction” — after receiving the Vero Cell COVID vaccine, authorized in May by the World Health Organization for emergency use.
Three Vietnamese children die after Pfizer vaccine
Vietnam on Nov. 30 rolled out its COVID vaccination program for children 15 to 17 years old with Pfizer’s vaccine. Since then, three children have died after receiving their first dose. The cause of death was “overreaction to the vaccine.”
One of the three deaths reported in Vietnam includes a 12-year-old boy in the southern province of Binh Phuoc who died one day after his first Pfizer shot.
The boy received his vaccine Monday afternoon and was sent home to rest. After dinner, he experienced dizziness, abdominal pain and diarrhea. He was taken to a local hospital and then transferred to two others, but died Tuesday morning.
The Binh Phuoc Department of Health set up an expert panel to determine the cause of the 12-year-old’s death.
A 16-year-old boy in the northern Bac Giang Province, and a ninth-grade girl in Hanoi, both died Sunday after receiving Pfizer’s COVID vaccine.
The Health Ministry said both deaths were caused by “overreaction to the vaccine,” not by a problem with the quality of the vaccine or the vaccination process.
Drugmakers Pfizer and Merck on Nov. 24 agreed to give licenses to firms in Vietnam to produce COVID treatment pills — paxlovid (Pfizer) and molnupiravir (Merck).
Vietnam is one of 95 low- and middle-income countries allowed to produce the pills through a voluntary licensing agreement with Medicines Patent Pool, an international public health group backed by the United Nations.
According to the latest data from the U.S. Vaccine Adverse Event Reporting System, there have been 18,558 reported adverse events following Pfizer’s COVID vaccine among 12 to 17-year-olds.
Moronic, Outgoing NYC Mayor Announces Mandatory Vaccine Requirement for All Private Employers w/No Testing Option. Businesses Cannot be Held Liable for Medical Harm that Results from a Mandatory Vax
/
From [HERE] Earlier today, NYC Mayor Bill de Blasio announced a first-in-the-nation vaccine mandate covering all private-sector workers in NYC that will take effect on December 27, 2021. According to Mayor de Blasio, the mandate will cover approximately 184,000 businesses.
NYC is set to publish guidelines for employers on December 15, which will provide employers with less than two weeks to implement and enforce the new mandate. Although we do not yet know the full scope of the new requirement, we anticipate that there will be few exceptions. We also anticipate that the mandate will be challenged in the courts. Mayor de Blasio announced that the mandate will apply to all in-person employees, and those employees will not have the option of getting regularly tested in lieu of vaccination. Employees must have at least one dose of the vaccine by December 27.
The mandate is slated to take effect just days before Mayor-elect Eric Adams replaces Mr. de Blasio.
“There’s no clarity around who and how this will be enforced,” Ms. Wylde said.
Evan Thies, a spokesman for Mr. Adams, said the mayor-elect would evaluate the mandate, as well as other Covid-19 strategies, when he takes office. [MORE]
Apparently the mandate will not make businesses liable for any medical harm that results from a mandatory vaccination.
It is undisputed that COVID “vaccines” do not prevent transmission or prevent individuals from getting COVID. A recent Harvard study shows no discernible relationship between the vaccination rate and new cases. Meanwhile, evidence in study after study has demonstrated that so-called COVID “vaccines” are extremely dangerous. Below professor Dr. Julie Ponesse raises several questions relevant to illogical mandates;
Consider these facts:
1) COVID-19 has an infection fatality rate not even 1% that of smallpox (and it poses even less risk to children)
2) a number of safe, highly effective pharmaceuticals exist to treat it (including monoclonal antibodies, Ivermectin, fluvoxamine, Vitamin D and Zinc), AND
3) The vaccines have reported more adverse events (including innumerable deaths) than every other vaccine on the market over the last 30 years.
In light of these facts, I have so many questions:
Why are the vaccinated granted vaccine passports and access to public spaces, when the Director of the CDC has stated that the COVID-19 vaccines cannot prevent transmission?
Why is vaccination the ONLY mitigation strategy when emerging evidence (including a recent Harvard study) shows no discernible relationship between the vaccination rate and new cases?
Why does our government continue to withhold Ivermectin as a recommended treatment when the U-S National Institutes of Health supports it, and when the state of Uttar Pradesh in India distributed it to its 230 million people, reducing its COVID death rate to almost zero? How has India surpassed Canada in Health Care?
Why are we about to vaccinate 5 year olds when COVID poses to them less risk than the potential vaccine reactions AND while there is NO effective monitoring system for the vaccines?
Why are we focused on the narrow benefits of vaccine-induced immunity when real-world studies show natural immunity is more protective, more potent, and more enduring?
Why do we shame the “vaccine hesitant” and not the “vaccine adamant”?
“Why,” as a nurse recently asked, “do the protected need to be protected from the unprotected by forcing the unprotected to use the protection that did not protect the protected in the first place?”
By every measure and from every angle, this is a ‘house of cards’ about to crumble
But the question that interests me is why hasn’t it crumbled already? Why are these questions not the headlines of every major newspaper in Canada every day? [MORE]
W/Low Vaccination Rates Africa’s Covid Deaths Remain Far Below Europe and US. According to WHO Data Deaths in Africa are Only 2.9% of Covid Deaths Worldwide while Africa is 16% of the World Population
/
From [GR] Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured that those jurisdictions that implement the lockdown would experience only a fraction of the death toll.
Then, once vaccines became available, the narrative was modified to:
“Get shots in arm and then covid will stop spreading. Those countries without vaccines, on the other hand, will continue to face mass casualties.”
The lockdown narrative, of course, has already been thoroughly overturned. Jurisdictions that did not lock down or adopted only weak and short lockdowns ended up with covid death tolls that were either similar to—or lesser than—death tolls in countries that adopted draconian lockdowns. Lockdown advocates said locked-down countries would be overwhelmingly better off. These people were clearly wrong.
Undaunted by the increasing implausibility of the lockdown narrative, the global health bureaucrats are nonetheless doubling down on forced vaccines—as we now see in Austria—and we continue to be assured that only countries with high vaccination rates can hope to avoid disastrous covid outcomes.
Yet, the experience in sub-Saharan Africa calls both these narratives into question: Africa’s numbers have been far, far lower than the experts warned would be the case.
For example, the AP reported mid November 2021 that in spite of low vaccination rates, Africa has fared better than most of the world:
[T]here is something “mysterious” going on in Africa that is puzzling scientists, said Wafaa El-Sadr, chair of global health at Columbia University. “Africa doesn’t have the vaccines and the resources to fight COVID-19 that they have in Europe and the U.S., but somehow they seem to be doing better,” she said….
Fewer than 6% of people in Africa are vaccinated. For months, the WHO has described Africa as “one of the least affected regions in the world” in its weekly pandemic reports.
Yet disaster for Africa has long been predicted for several reasons even beyond the availability of vaccines. For instance, it is known that lockdowns are especially impractical in the poorest parts of the world. This is because populations in places with underdeveloped economies can’t simply sit at home and live off savings or debt. Rather, these people must go out into the world and earn a living on a day-to-day basis. Starvation is the alternative. Moreover, much of this work is done in the informal economy, so enforcing lockdowns becomes especially difficult.
It was also assumed that covid would be especially deadly in Africa due to the fact many large households live in small housing units.
But that “conventional wisdom” flies in the face of the reality of covid in Africa, which is that there have been fewer deaths.
The “experts” have groped around, looking for possible explanations.
Some sources, for example, insist that the low death totals are only an artifact of incomplete reporting on covid infections and that “a lack of good qualitative data was the issue.”
But Richard Wamai at Northeastern University rejects the claim it’s all about case reporting, and says that “local systems for reporting deaths in Africa make it difficult to hide COVID-19 casualties.” In a paper for the International Journal of Environmental Research and Public Health, Wamai and his coauthors conclude,
“[T]here is no evidence that COVID-19 mortality data is less accurately reported in Africa than elsewhere” …
“While the true picture of infections and mortality in the continent has yet to fully emerge, the quality of data for other diseases, such as HIV/AIDS, indicates that Africa has the capacity to collect and report valid disease surveillance data.”
In any case, the World Health Organization reports that covid deaths in Africa make up only 2.9 percent of covid deaths Worldwide, while Africa’s population is 16 percent of the global total.
Africa’s covid total could double or triple, and Africa would still be faring far better than Europe and the Americas.
Wamai et al. also note that at this point
“[i]t is likely that SARS-CoV-2 has already been widely disseminated through Africa…. If so, widespread infection is likely to also result in widespread natural immunity.”
In other words, continued claims by health officials—both in Africa and elsewhere—that mass death is right around the corner with the “next wave” look increasingly implausible.
It looks increasingly likely that the lack of covid mortality in Africa is not due to a data issue nor a situation in which covid has been “contained” up until now. So then why is Africa doing so much better than the wealthy West?
Naturally, the advocates of forced lockdowns and coerced vaccines would prefer to ignore this issue altogether, but the undeniable reality of Africa’s experience has forced mainstream researchers to publicly admit the many ways that many factors can explain covid’s prevalence beyond vaccination rates and mask mandates.
For instance, mentioning that obesity is an important factor in covid mortality has in the past been likely to get one savaged in the media for “fat shaming.” Yet the Africa situation has forced the well informed to admit that yes, obese populations clearly suffer more from covid. In Africa, not surprisingly, we find that obesity rates are far below those found in North America and Europe.
Other possible explanations forwarded as reasons for Africa’s situation include past exposure to other coronaviruses, youthful populations, fewer patients lacking zinc and vitamin D, past use of the Bacillus Calmette-Guérin vaccination, climate, genetic background, and parasite load.
In addressing the African “enigma” one group of researchers in the journal Colombia medica dared even suggest it’s possible—although not conclusively shown at this point—that “a mass public health preventive campaign against COVID-19 may have taken place, inadvertently, in some African countries with massive community ivermectin use.”
In the West, however, the media drumbeat around covid has consistently been “Shut up, stay home, get jabbed, and stop doubting the experts on forced vaccines.” Fortunately, however, the African situation has forced many researchers to ask inconvenient questions.
In fact, it’s amazing Africa has not been overcome by mass death considering that covid lockdowns and covid economic and social “mitigation” measures have contributed to the impoverishment and mass starvation on the continent. Or as Germany’s DW News puts it,
“Measures put in place to slow the spread of the novel coronavirus are pushing millions of people in Africa into severe hunger.”
And as Wamai notes,
“[S]ome of the excess deaths in Africa “can be attributed not to the disease, but to lockdown measures that cut off access to medical care for other illnesses.”
But Africa hasn’t gotten the bloodbath that was promised, and as one Nigerian put it, “They said there will be dead bodies on the streets and all that, but nothing like that happened.”
LeBron James Cleared to Return After Meaningless PCR Covid Tests Say So [never in the history of Respiratory Disease have Healthy People with No Symptoms Spread a Deadly Virus- COVID is a Mind Virus]
/MAKES GOOD SENSE TO SHEEPLE. From [HERE] Two days after LeBron James was sidelined by the league’s health and safety protocols because he registered conflicting Covid-19 results, the NBA’s biggest star is back after the league said that subsequent testing determined that he was not a positive case.
James, who is fully vaccinated, was ruled out indefinitely on Tuesday after he tested positive for Covid in a sample collected on Monday, according to the NBA, which issued a statement outlining his testing results in unusual detail on Thursday night.
The league said that Monday’s positive sample was tested again Tuesday on two different PCR machines and returned one positive result and one negative result, prompting James to miss the Lakers’ game that night and return to Los Angeles amid the uncertainty. He then underwent two more rounds of testing on Tuesday, which only added to the confusion, as he returned one negative and one “clinically inconclusive” result, the league said.
He was cleared to return to the court when James registered negative PCR tests on Wednesday and Thursday, according to a person familiar with the matter.
The league’s vaccinated players who test positive must remain out for at least 10 days or, in James’s case, until they return two negative results at least 24 hours apart. [MORE]

IN REALITY THE VESTED INTERESTS ARE FUCKING WITH YOUR MIND. it is undisputed that the PCR tests don’t work to diagnose active infection with covid19.
We all keep saying that don’t we, but we don’t seem able to grasp what it means, because even though we know PCR tests don’t work to diagnose infection we keep accepting all the statistics that are produced as a result of assuming PCR tests diagnose infection.
We say – “0h wow, covid numbers rising despite the lockdown”. Or “massive spike in people getting covid in THIS care home despite precautions”. Or “look the ‘vax’ doesn’t work because people who get it still catch covid”.
No. Wrong. They’re not “covid numbers”, they’re positive-test numbers. It’s not a spike in people ‘getting Covid’ in the care home, it’s a spike of people testing positive. The people who get the vax don’t “still catch covid”, they still test positive.
And the reason why these ‘anomalies’ happen, the reason why vaxxed people can still test positive, etc etc is the same reason a papaya can test positive – because the PCR tests don’t work.
We know it but keep forgetting it. So let’s say it again.
The PCR tests don’t work.
The PCR tests. Don’t. Work.
We all know the danger of false positives if too many cycles are run. This is admitted even by Fauci.
If you run your tests at 30 cycles or more the results are very likely to be junk and any positives meaningless. And, incredibly, most labs performing these tests have been doing just that – running cycles of 30 or more, even up to 45.
But this well known and important fact hides the even more important fact that even when the tests are done properly they still don’t work – in that they are not designed to do what they are being used for.
They don’t diagnose infection or detect active infection. They aren’t, for the most part, even specific for SARSCOV2. They just look to see if you have some random fragments of RNA in your body that someone has identified as being similar to some types of assumed viral RNA. [MORE]
It is a lie that People with No Symptoms Can Spread a Virus
"So-called asymptomatic cases have never in the history of respiratory disease been the driver for spread of infection. Rather it is symptomatic people who spread respiratory infections - not asymptomatic people" - https://worlddoctorsalliance.com/
This lie states that healthy people with no symptoms can spread a deadly virus, seriously. This lie keeps us all afraid of each other and makes people wear masks. We all have to then assume that every person you see could have the virus unknowingly, without symptoms and be spreading it..
Imagine if you go back to the normal year of 2019 and you explained you couldn’t go for a night out with a friend because you had the flu and you don’t want to give it to your friend your friend asked ‘oh I see, have you got aching muscles and temperature and you feel unwell’ and you said ‘no, I have no symptoms and I feel fine’. Your friend would laugh at you and would think you’re crazy. Hundreds of years of science have just been turned on its head.
So ask yourself if you go back to 2019 and all the decades before would you be scared of catching the flu of someone who has no symptoms of the flu. No you wouldn't. Covid-19 does not spread differently as it has the same symptoms as a coronavirus or the flu. But that is the lie we are being told by adverts on T.V and the radio and governments.
Nearly 10 million people were tested in Wuhan, consisting of 92 percent of all residents aged six years or older. Incredibly, no new symptomatic cases were registered, and only 300 asymptomatic cases were detected. Subsequent tests of 1,174 close contacts of the asymptomatic cases found resulted in no new positives. There is “no evidence that the identified asymptomatic positive cases were infectious,” the study said. [MORE]
Mass Vax was Supposed to Reduce the Number of Hospitalizations and Deaths, but Deaths Continue to Rise. Since Summer there have been 2X as many Covid Deaths and 7X as Many Excess Deaths as 2020 [UK]
/
From [HERE]
“Americans are scared to death…. People are walking off the job, not because they want to lose their jobs, but they don’t want to die from the vaccine! … They say, ‘Listen, I don’t want to die. That’s the reason I’m not taking the vaccine.’ It’s that clear.” Dr. Peter McCullough
A report in the U.K. Telegraph explains how the Covid-19 vaccine has led to a sharp rise in excess deaths. Here’s an excerpt from the article:
“Nearly 10,000 more people than usual have died in the past four months from non-Covid reasons, as experts called for an urgent government inquiry into whether the deaths were preventable….
Latest figures from the Office for National Statistics showed that England and Wales registered 20,823 more deaths than the five-year average in the past 18 weeks. Only 11,531 deaths involved Covid.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph)
Mortality is rising because more people are dying. And more people are dying because more people have been vaccinated. There’s a link between rising mortality and the Covid-19 vaccine. Naturally, the media wants to shift responsibility for the fatalities to “delayed treatments” and “the lack of preventable care”. But this is just a diversion. The primary cause of death is the injection of a toxic pathogen into the bloodstreams of roughly 70% of the population. That’s what’s causing the clotting, the bleeding, the pulmonary embolisms, the heart attacks, the strokes, and the premature deaths. It’s the vaccine. Here’s more
“Weekly figures for the week ending November 5 showed that there were 1,659 more deaths than would normally be expected at this time of year. Of those, 700 were not caused by Covid.
The excess is likely to grow as more deaths are registered in the coming weeks.
Data from the UK Health Security Agency show there have been thousands more deaths than the five-year average in heart failure, heart disease, circulatory conditions and diabetes since the summer.

The number of deaths in private homes is also 40.9 per cent above the five-year average, with 964 excess deaths recorded in the most recent week, which runs up to November 5.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph)
The sudden surge in mortality is not a meaningless blip on the radar. It’s a red flag indicating a significant break in the five-year trend. Something has gone terribly wrong. Mass vaccination was supposed to reduce the number of cases, hospitalizations and deaths. Instead, the fatalities continue to rise.
Why?
The answer to that question can be found in the data itself. As the author admits, there has been a sharp uptick in heart failure, heart disease, circulatory conditions and strokes. (Diabetes is the outlier) These are precisely the ailments one would expect to see if one had just injected millions of people with a clot-generating biologic that triggers a violent immune response that attacks the inner lining of the blood vessels inflicting severe damage to the body’s critical infrastructure. So, yes, all-cause mortality is up, and it is certain to climb even higher as more people are vaccinated and gradually succumb to the (frequently) delayed effects of a hybrid concoction that is the cornerstone of a malign plan to dramatically reduce global population. Check out this chart followed by a brief comment by diagnostic pathologist, Dr Claire Craig:
Dr Clare Craig @ClareCraigPath
“Since summer there have been twice as many covid deaths, but seven times as many excess deaths as last year.” (Twitter)
And here’s another blurb from Craig:
“If you start at week 22 and add up all the deaths since for each year, then something very abnormal is happening this year among 15-19 yr old males.”
So, not only are more people dying, but the demographic has shifted downwards as younger and younger people are drawn into the vaccine vortex. Simply put, the number of young people dying from vaccine-inflicted cardiac arrest and myocarditis continues to increase with no end in sight.
Not surprisingly, all-cause mortality is higher among the vaccinated than the unvaccinated which, again, makes it easier to trace the problem back to its root, a cytotoxic “poison-death shot” that suppresses the innate immune system, damages vital organs and shaves years off the lives of normal, healthy people.
Perhaps, you’ve seen one of the many short videos of fit, young athletes who suddenly have dropped dead on the field of play or been rushed to hospital shortly after getting injected. If not, here’s a link to two of them. (Athletes collapse following vaccination: See here and here)
According to Israeli Real-Time News, there has been a “500% increase in deaths of players in 2021… Since December, 183 professional athletes and coaches have suddenly collapsed! 108 of them died!”
“500% increase in the deaths” of athletes?!? What are we to make of this?
For starters; the Covid-19 vaccine is not a medication. It is the essential component in the elitist plan for industrial-scale extermination. It is designed to inflict severe physical injury on the people who take it. It’s shocking that people are so deep in denial that can’t see what’s going on right before their eyes. (Please, watch the video clips of the athletes. These are the fittest people on the planet and, yet, they are being struck down by the mystery substance in the vaccine.) Here’s how South African doctor Shankara Chetty summed it up in a recent video posted on Bitchute:
“The pathogen that is causing all the deaths from the illness is the spike protein. And the spike protein is what the vaccine is supposed to make in your body. …Spike protein is one of the most contrived poisons that man has ever made. And, the aim of this toxin, is to kill billions of people without anyone noticing it. So it is a poison with an agenda.” (“South African Physician Dr. Shankara Chetty Talks about “The Bigger Plan”, Bitchute)
There it is in a nutshell. And Chetty is not alone in linking the vaccine to the agenda of the globalist elites who plan to use the cover of a pandemic to implement their “population management” scheme. Former Pfizer vice president, Mike Yeadon, offered a similar view just days ago on his website. He said:
“We are in the midst of the biggest depopulation program the world has ever seen, where most of humanity are acting as useful idiots to it and to their own demise.”
Indeed, and we have tried to provide as much information as possible on the biologic agent that is being used to pursue this malign agenda, the spike protein. In early reports we passed along the research of Dr. Patrick Whelan who grasped the danger of the spike protein before anyone else. Here’s a brief recap of his analysis from a letter he submitted to the FDA on December 8, 2020:
“I am concerned about the possibility that the new vaccines aimed at creating immunity against the SARS-CoV-2 spike protein have the potential to cause microvascular injury to the brain, heart, liver, and kidneys in a way that does not currently appear to be assessed in safety trials of these potential drugs.
… Meinhardt et al…. show that the spike protein in brain endothelial cells is associated with formation of microthrombi (clots)… In other words, viral proteins appear to cause tissue damage without actively replicating virus…. The Pfizer/BioNTech vaccine (BNT162b2) is composed of an mRNA that produces a membrane-anchored full-length spike protein. The mouse studies suggest that an untruncated form of the S1 protein like this may cause a microvasculopathy in tissues that express much ACE2 receptor.
…it appears that the viral spike protein… is also one of the key agents causing the damage to distant organs that may include the brain, heart, lung, and kidney. Before any of these vaccines are approved for widespread use in humans, it is important to assess in vaccinated subjects the effects of vaccination on the heart…. As important as it is to quickly arrest the spread of the virus by immunizing the population, it would be vastly worse if hundreds of millions of people were to suffer long-lasting or even permanent damage to their brain or heart microvasculature as a result of failing to appreciate in the short-term an unintended effect of full-length spike protein-based vaccines on these other organs. (“FDA shrugs off dire warning about lethal spike protein“, Truth in the Age of Covid)
From the very beginning, government regulators and their allies in public health establishment have ignored (or censored) the warnings of capable physicians and researchers. They also waved-off career immunologist and vaccinologist, Dr Byram Bridle who was the first in his profession to identify the spike protein as “a specific causative agent of disease”; aka–“a pathogen”. Here’s Bridle:
“‘We have known for a long time that the spike protein is pathogenic…. It is a toxin. It can cause damage in our body if it’s in circulation. Now, we have clear-cut evidence that . . . the vaccine itself, plus the protein, gets into blood circulation.’”
Once that happens, the spike protein can combine with receptors on blood platelets and with cells that line our blood vessels. This is why, paradoxically, it can cause both blood clotting and bleeding. ‘And of course the heart is involved, as part of the cardiovascular system… That’s why we’re seeing heart problems. The protein can also cross the blood-brain barrier and cause neurological damage.…
‘In short,… we made a big mistake. We didn’t realize it until now. We didn’t realize that by vaccinating people we are inadvertently inoculating them with a toxin.”… (“Vaccine scientist: ‘We’ve made a big mistake’“, Conservative Woman)
Here again, we have a highly-regarded immunologist, with more than 3 decades of experience under his belt, who offered his informed and evidence-based research on an issue that should have been of great interest to the regulators that were making decisions about the long-term safety of the experimental drug they were foisting on millions of people across the country. But there was no interest at all. Despite the fact that the science supported his conclusions, Bridle was viciously attacked, censored, dragged through the mud, and forced to leave his place of employment.
Why?
Because he drew the same conclusions as Dr. Patrick Whelan. There’s really no substantive difference between the two except that Bridle’s comments attracted more attention in the media which made him a greater threat to the “universal vaccination” strategy. That was his real crime; he discovered the truth and made his findings available to the public, basically alerting them to the dangers of the “poison-death shot”. For that he was crushed.
Bridle has since made other claims that should concern anyone whose cancer might be in remission. Here’s what he said in a recent interview:
“What I’ve seen way too much of is people who had cancers that were in remission, or that were being well controlled; their cancers have gone completely out of control after getting this vaccine. And we know the vaccine causes a drop in T-cell numbers, and those T-cells are part of our immune system and they are part of the critical weapons our immune system has to fight off cancer cells; so there’s a potential mechanism there. All I can say, is I’ve had way too many people contact me with these reports for me to feel comfortable. I would say that is my newest major safety concern, and it’s also the one that’s going to be the most under-reported in the adverse data base, because if someone has had cancer before the vaccine, there’s no way public health officials will ever link it to the vaccine.” (“Dr Byram Bridle speaks”, Bitchute, :55 second-mark)
So, the vaccine suppresses the immune system?
Yes, it does, and author Alex Berenson provided evidence of this just recently in an article he posted on Substack. Here’s an excerpt:
“… the British government…. admitted today, in its newest vaccine surveillance report, that:
“N antibody levels appear to be lower in people who acquire infection following two doses of vaccination.” (Page 23)
What’s this mean?…
What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus….
This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE…
it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.” (“URGENT: Covid vaccines will keep you from acquiring full immunity EVEN IF YOU ARE INFECTED AND RECOVER”, Alex Berenson, Substack)
Berenson’s observations square with research that was compiled earlier in the year by scientists in The Netherlands and Germany who:
“….warned that the … (COVID-19) vaccine induces complex reprogramming of innate immune responses that should be considered in the development and use of mRNA-based vaccines… the research team from Radboud University Medical Center and Erasmus MC in the Netherlands… showed that the vaccine altered the production of inflammatory cytokines by innate immune cells following stimulation with both specific (SARS-CoV-2) and non-specific stimuli.
Following vaccination, innate immune cells had a reduced response to toll-like receptor 4 (TLR4), TLR7 and TLR8 – all ligands that play an important role in the immune response to viral infection…. an unexplored area is whether BNT162b2 vaccination has long-term effects on innate immune responses …
This could be very relevant in COVID-19, in which dysregulated inflammation plays an important role in the pathogenesis and severity of the disease,” writes the team. “Multiple studies have shown that long-term innate immune responses can be either increased (trained immunity) or down-regulated (innate immune tolerance) after certain vaccines or infections.” (Research suggests Pfizer-BioNTech COVID-19 vaccine reprograms innate immune responses, new-medical-net)
Berenson’s finding also align with with cutting-edge research showing that the spike protein greatly “impedes adaptive immunity” by preventing DNA from repairing damaged cells. The paper suggests that the spike protein does in fact “impact on the nucleus of the cell, where we store our DNA, our core genetic material.” Here’s more from Berenson’s breakdown of the paper:
“…. our cells have mechanisms to repair their own DNA.
But – at least in the experiments these two scientists ran – the spike protein appeared to interfere with our own DNA repair proteins: “Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site.”
To be clear, the scientists did NOT prove the spike protein was causing these problems in people, or even animals… Nonetheless, at a time when advanced countries that have high mRNA (and DNA/AAV) vaccination rates are seeing unusually full hospitals and higher-than-normal death rates, they are yet more cause for concern. As the authors explained:
“Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.” (“URGENT: Worrisome paper about the spike protein’s impact on DNA and DNA repair”, Alex Berenson, Substack)
Bottom line: If the vaccine does in fact inhibit the body’s innate immune response, then people are going to get alot sicker from seasonal infections that routinely spread through the population. Their path to recovery will also be alot more difficult.
But rather that belabor the immunity angle, let’s move on to the research of Dr Charles Hoffe who was the first physician to provide hard evidence that the vaccines generate blood clots by triggering an immune response in which the body attacks the thin layer of cells lining the walls of the blood vessels. Hoffe found that 62% of his patients that had been vaccinated tested positive for blood clots on a D-dimer test. Naturally, he was alarmed by what he found, particularly since the vaccine “was causing serious neurological events, and even death.When he raised his concerns with the BC College of Physicians, they immediately implemented a gag order, and reprimanded him in an attempt to intimidate, and silence him.”
Hoffe has been interviewed a number of times and always provides a detailed and riveting account of his findings. In a recent interview, he predicted that some vaccinees suffering from clot-related issues would likely die in just three years. Here’s what he said:
“… once you block off a significant number of blood vessels to your lungs, your heart must pump at a much greater resistance to get the blood through your lungs. That causes a condition called pulmonary artery hypertension, which is high blood pressure in your lungs because so many of the blood vessels in your lungs are blocked. And the terrifying thing about this is tha t people with pulmonary artery hypertension usually die of right-sided heart failure in three years… And not only is the long-term outlook very grim, but with each successive shot, the damage will add and add and add. It’s going to be cumulative because you are getting more and more damaged capillaries.” (“Shock: Doctor Warns That Majority Of Vaccinated Patients Could HavePermanent Heart Damage, Some May Die Within Three Years”Permanent Heart Damage, Some May Die Within Three Years”, Infowars; Minute 6:10)
Once again, there is no discrepancy between the analysis of Whelan, Bridle and Hoffe. And while the focus of their attention might vary slightly, their conclusions are the same. These experimental injections pose serious risks for anyone who allows himself to be inoculated.
Now check out how similar Hoffe’s analysis is to Dr. Rochagne Kilian who was an Emergency Room physician at the GBHS hospital until she resigned in protest. This is a particularly important video as it describes the “oddball” symptoms and exceedingly rare conditions that are now presenting in emergency rooms everywhere following the mass vaccination of millions of people with the “poison-death shot”. (I transcribed the video myself, so there could be errors.)
Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels
“What I was seeing in my ER department especially in the last 8 to 9 months is related to the D-Dimer levels. We use D-Dimers specifically related to pulmonary embolisms as well as Deep Vein Thrombosis. D-Dimer detects any thrombosis (clots) in the body but it doesn’t give you a diagnosis it gives you a basis for going further and doing an ultrasound and CT scan to either confirm or deny the presence of a pulmonary embolism or Deep Vein Thrombosis.
The first part of 2020 was probably the slowest ever in the emergency department, but when we went into 2021 and the vaccination rollout started, we ended up seeing an increase in stroke, transient ischemic attacks and stroke like presentations. (There were) definitely significant larger numbers of those people coming in. I ended up doing D-dimer tests on these people and never before in my clinical experience had I seen D-dimers and the amount of people with positive D-dimers higher than 2,000, higher than 3,000 and higher than 5,000. My clinical experience told me a needed to go look for a large clot either in their legs or their lungs. And I ended up doing a CT scan on these people. Most of them, and I will say almost all of them, had negative scans which started making me think that if there was not a significant clot in their lungs, but my D-dimer was so much higher than what I was usually seeing, it might not be concentrated in one clot. But that it is multiple micro-thrombi extended throughout the body, and that is so easy to miss because the CT scan is not going to pick it up.
“These people coming into the ER were all people anywhere from about a week to four months after receiving their 2nd injections. There are certain factors that can influence a D-dimer test that can give you a sense of a higher level than would be expected in the body. That said, the patients I was doing D-Dimer tests on did not have a level of maybe a positive 500 or 400 reading. It was more than 3500, more than 5000 ng/ml. So those are significantly positive without any proof of having a pulmonary embolism. If I was seeing high levels of D-dimer without a definite diagnosis, I needed to ask more questions.
One study said, never ignore extremely elevated D-dimer levels. They are specific for serious illness, including venous thrombosis, sepsis, and/or cancer. Even if sharply elevated D-dimer are a seemingly solitary finding, clinical suspicion of severe underlying disease should be maintained.
There were two conditions that stood out and the first one was disseminated intravascular coagulation also known as DIC. The second one is antiphosphlipid syndrome. Both of these conditions are related to an abnormality in either the initiation or the feedback of the coagulation pathway as well as thrombosis or the thrombosis cycle where clots are being broken down. DIC is a serious sometimes life threatening situation in which the proteins in the blood involved in blood clotting become overactive. It’s a cascade that’s difficult to stop once it’s reached a certain level. There are certain conditions that trigger DIC; significant sepsis, underlying viruses, trauma, major surgery, pregnancy and childbirth. And less common causes toxic drug reaction, blood transfusion reaction, and organ transplants. So there was a connection with intravascular products and a possible DIC.
Most cases of DIC are diagnosed rapidly and suddenly which is the acute presentation. But there are cases where it develops gradually, occurring over a longer period of time. This is known as a chronic form of DIC and I would go as far to say a subacute form of DIC that is very easy to miss. Simultaneous clotting and bleeding can occur with chronic DIC. The bleeding part comes in blood in the urine, headaches and other symptoms associated with brain bleeds, bruising, inflammation of red, small dots on the limbs, bleeding at sites of wounds and mucosal bleeding. which means bleeding out of the gums and nose. I definitely saw an increase in nose bleeds and bleeding from previous wound sites. ulcers, as well as rashes that couldn’t be explained. Blood clotting symptoms and signs were symptoms like chest pains, heart attacks, strokes, TIAs, and headaches either related to bleeding or not. As well as symptoms related to kidney failure, because of the clotting of those smaller blood vessels that go to the kidneys. Antiphosphlipid syndrome is a very similar type of condition. But the basis of the antiphosphlipid syndrome is an autoimmune disorder meaning that the body’s immune system makes proteins–known as antibodies–that mistakenly attacks its own body or tissues. That gives the skin the cascading effect of clotting disorder but it is linked to an autoimmune trigger. Basically, it presented in exactly the same way; high blood pressure which I was seeing alot of; first diagnosis of high blood pressure, heart attacks, strokes, TIAs, heart valve problems, repeated headaches or migraines, vision loss, balance and mobility problems, difficulty concentrating or thinking clearly,
The astute listener would start forming a picture of what we’ve been told about Covid-19, and there are research papers connecting Covid 19 with an underlying vascular disease. One of these was a study called “Covid 19; unraveling the clinical progression of Nature’s Virtually perfect Biological weapon.”
“SARS-Cov-2, presenting as Covid-19 syndrome, was not a respiratory basis, but an underlying vascular basis. which had certain phases of incubation, pulmonary phase, pro inflammatory phase, (which once again comes into a cytotoxic inflammation process) then moves into a protothrombic phase . Covid-19 is a thrombotic disease. implications for prevention, antithrombotic therapy and follow up…..
This picture shows us certain risk factors, Homeostatic Abnormalities, as well as clinical outcomes. It indicates increased D-dimer levels. It also mentions Venous Thromboembolism, Myocardial Infarction, and Disseminated Intravascular Coagulation that is connected to postulated mechanisms of coagulathopy as well as parthenogenesis of thrombosis in Covid-19…
I started asking the question, if we are able to detect certain connections between vascular abnormalities and Covid-19, and we based our proposed treatment on the spike protein, which includes the Pfizer and Moderna injections, shouldn’t we be looking for similar side effects or complications from that same injection?
If we are mandating certain treatments, we do need to do the due diligence to make sure what the side effects and complications especially in a time where there has not been long term studies.”And that’s what led me to focusing on D-dimers.” (“Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels“, Bitchute)
Kilian’s statement should be read over and over again. It is the most detailed description we have of the mysterious and deeply sinister machinations of a laboratory-engineered bioweapon that, in effect, turns the vascular and immune systems against the person who was vaccinated. Disseminated intravascular coagulation and antiphosphlipid syndrome are names that are entirely unknown to the American people, and yet, these freakish conditions are now responsible for a growing number of patients that are experiencing bleeding, clotting, headaches, rashes, bruising, high blood pressure, and inflammation . And– in more extreme cases– chest pains, heart attacks, strokes, heart-valve problems, and brain bleeds. One can only guess how the media will try to cover-up these extraordinarily-rare and potentially life-threatening conditions?? [MORE]
The COVID Injection isn't a Vaccine, It’s a Bioweapon Made in 1999, Later Perfected, Weaponized and Patented as a Deadly Spike Protein. Underwriter David Martin has The Receipts and Patent Numbers
/Dr. David E. Martin is the Founder and Chairman of M·CAM Inc., an international leader in innovation finance, trade, and intangible asset finance. M.CAM is a Virginia-based company that underwrites lending on intellectual property, earning a fee from the lender, usually a bank, and in most cases the right to sell on the IP if the company defaults. [MORE] Martin is the developer of the first innovation-based quantitative index of public equities and is the Managing Partner of the Purple Bridge Funds. He is the creator of the world’s first quantitative public equity index – the CNBC IQ100 powered by M·CAM. He is also a respected financial analyst. [MORE]
The Fauci/COVID-19 Dossier
This document is prepared for humanity by Dr. David E. Martin.
Over the past two decades, my company- M.CAM - has been monitoring possible violations of the 1925 Protocol for the Prohibition of the Use in War of Asphyxiating, Poisonous, or other Gases, and of Bacteriological Methods of Warfare (the Geneva Protocol) 1972 Convention on the Prohibition of the Development, Production, and Stockpiling of Bacteriological and Toxin Weapons and Their Destruction (the BTWC). In our 2003-2004 Global Technology
Assessment: Vector Weoponizotion M.CAM highlighted China's growing involvement in Polymerase Chain Reaction (PCR) technology with respect to joining the world stage in chimeric construction of viral vectors. Since that time, on a
weekly basis, we have monitored the development of research and commercial efforts in this field, including, but not limited to, the research synergies forming between the United States Centers for Disease Control and Prevention (CDC),
the National Institutes for Allergies and Infectious Diseases (NIAID), the University of North Carolina at Chapel Hill (UNC), Harvard University, Emory University, Vanderbilt University, Tsinghua University, University of Pennsylvania, many other research institutions, and their commercial affiliations.
The National Institute of Health's grant AI23946-08 issued to Dr. Ralph Baric at the University of North Carolina at Chapel Hill (officially classified as affiliated with Dr. Anthony Fauci's NIAID by at least 2003) began the work on synthetically altering the Coronaviridae (the coronavirus family) for the express purpose of general research, pathogenic enhancement, detection, manipulation, and potential therapeutic interventions targeting the same. As early as May 21, 2000, Dr. Baric and UNC sought to patent critical sections of the coronavirus family for their commercial benefit.1 In one of the several papers derived from work sponsored by this grant, Dr. Baric published what he reported to be the full length cDNA of SARS CoV in which it was clearly stated that SAR CoV was based on a composite of DNA segments.
"Using a panel of contiguous cDNAs that span the entire genome, we have assembled a full-length cDNA of the 5ARS-CoV Urbani strain, and have rescued molecularly cloned 5AR5 viruses (infectious clone 5ARS-CoV) that contained the expected marker mutations inserted into the component clones. ,2
On April 19, 2002 -the Spring before the first SARS outbreak in Asia - Christopher M. Curtis, Boyd Yount, and Ralph Baric filed an application for U.S. Patent 7,279,372 for a method of producing recombinant coronavirus. In the first public record of the claims, they sought to patent a means of producing, "an infectious, replication defective, coronavirus." This work was supported by the NIH grant referenced above and GM63228. In short, the U.S. Department of Health and Human Services was involved in the funding of amplifying the infectious nature of coronavirus between 1999 and 2002 before SARS was ever detected in humans.
Against this backdrop, we noted the unusual patent prosecution efforts of the CDC, when on April 25, 2003 they sought to patent the SARS coronavirus isolated from humans that had reportedly transferred to humans during the 2002-2003 SARS outbreak in Asia. 35 U.S.C. §202 prohibits patenting nature. This legality did not deter CDC in their efforts. Their application, updated in 2007, ultimately issued as U.S. Patent 7,220,852 and constrained anyone not licensed by their patent from manipulating SARS CoV, developing tests or kits to measure SARS coronavirus in humans or working with their patented virus for therapeutic use. Work associated with this virus by their select collaborators included considerable amounts of chimeric engineering, gain-of-function studies, viral characterization, detection, treatment (both vaccine and therapeutic intervention), and weaponization inquiries.
In short, with Baric's U.S. Patent 6,593,222 (Claims 2 and 5) and CDC's '852 patent (Claim 2), no research in the United States could be conducted without permission or infringement.
We noted that gain-of-function specialist, Dr. Ralph Baric, was both the recipient of millions of dollars of U.S. research grants from several federal agencies but also sat on the World Health Organization's International Committee on Taxonomy of Viruses (ICTV) and the Coronaviridae Study Group (CSG). In this capacity, he was both responsible for determining "novelty" of clades of virus species but directly benefitted from determining declarations of novelty in the form of new research funding authorizations and associated patenting and commercial collaboration. Together with CDC, NIAID, WHO, academic and commercial parties (including Johnson & Johnson; Sanofi and their several coronavirus patent holding biotech companies; Moderna; Ridgeback; Gilead; Sherlock Biosciences; and, others), a powerful group of interests constituted what we would suggest are "interlocking directorates" under U.S. anti-trust laws.
These entities also were affiliated with the WHO's Global Preparedness Monitoring Board (GPMB) whose members were instrumental in the Open Philanthropy-funded global coronavirus pandemic "desk-top" exercise EVENT 202 in October 2029. This event, funded by the principal investor in Sherlock Biosciences and linking interlocking funding partner, the Bill and Melinda Gates Foundation into the GPMB mandate for a respiratory disease global preparedness exercise to be completed by September 2020 alerted us to anticipate an "epidemic" scenario. We expected to see such a scenario emerge from Wuhan or Guangdong China, northern Italy, Seattle, New York or a combination thereof, as Dr. Zhengli Shi and Dr. Baric's work on zoonotic transmission of coronavirus identified overlapping mutations in coronavirus in bat populations located in these areas.
This dossier is by no means exhaustive. It is, however, indicative the numerous criminal violations that may be associated with the COVlD-29 terrorism. All source materials are referenced herein. An additional detailed breakdown of all the of individuals, research institutions, foundations, funding sources, and commercial enterprises can be accessed upon request.
35 U.S.C. § 101
From Justice Clarence Thomas' opinion for the majority
Section 101 of the Potent Act provides: "Whoever invents or discovers any new and useful.., composition of matter, or any new and useful improvement thereof, may obtain a potent therefor, subject to the conditions and requirements of this title."35 U.S.C. § 101.
We have "long held that this provision contains an important implicit exception[:] Laws of nature, natural phenomena, and abstract ideas ore not patentable." Mayo, 566 U.S., at_~, 132 S. Ct., at 1293 (internal quotation marks and brackets omitted). Rather, "'they ore the basic tools of scientific and technological work'" that lie beyond the domain of patent protection. Id., at ~ 132 S.Ct., at 1293. As the Court has explained, without this exception, there would be considerable danger that the grant of patents would "tie up" the use of such tools and thereby "inhibit future innovation premised upon them." Id., at ~ 132 S.Ct., at 1301. This would be at odds with the very point of patents, which exist to promote creation. Diamond v. Chakrabarty, 447 U.S. 303, 309, 100 S.Ct. 2204, 65 L.Ed.2d 144 (1980) (Products of nature ore not created, and "'manifestations... of nature [ore]free to all men and reserved exclusively to none'").3
In their majority opinion in 2013, the U.S. Supreme Court made it abundantly clear that the Court had "long held" that nature was not patentable. Merely isolating DNA does not constitute patentable subject matter. In their patent, the CDC made false and misleading claims to the United States Patent & Trademark Office by stating that, "A newly isolated human coronavirus has been identified as the causative agent of SARS, and is termed SARS-CoV."4 No "causal" data was provided for this statement.
When they filed their patent application on April 25, 2003 their first claim (and the only one that survived to ultimate issuance over the objection of the patent examiner in 2006 and 2007) was the genome for SARS CoV.
While this patent is clearly illegal under 35 U.S.C. §101, not only did the CDC insist on its granting over non-final and final rejections, but they also continued to pay maintenance fees on the patent after the 2013 Supreme Court decision confirmed that it was illegal.
In addition, the CDC patented the detection of SARS CoV using a number of methods including reverse transcription polymerase chain reaction (RT-PCR). With this patent, they precluded anyone outside of their licensed or conspiring interest from legally engaging in independent verification of their claim that they had isolated a virus, that it was a causative agent for SARS, or that any therapy could be effective against the reported pathogen.
It is important to note that the CDC's patent applications were also rejected in non-final and final rejections for ineligibility under 35 U.S.C. § 102 for being publicly disclosed prior to their own filing. In the first non-final rejection, the USPTO stated that the CDC's genome was published in four Genbank accession entries on April 14, 18, and 21, 2003 with identity ranging from 96.8% to 99.9% identical sequences,s Dr. Fauci knew, and failed to disclose evidence that the CDC patent was illegal, based on work he had funded in the years leading up to the SARS outbreak.

After seeking an illegal patent, petitioning to override the decision of an examiner to reject it, and ultimately prevailing with the patent's grant, the CDC lied to the public by stating they were controlling the patent so that it would be "publicly available".6 Tragically, this public statement is falsified by the simple fact that their own publication in Genbank had, in fact, made it public domain and thereby unpatentable. This fact, confirmed by patent examiners, was overridden by CDC in a paid solicitation to override the law.
While not covered under 35 U.S.C. §101, Dr. Fauci's abuse of the patent law is detailed below. Of note, however, is his willful and deceptive use of the term "vaccine" in patents and public pronouncements to pervert the meaning of the term for the manipulation of the public.
In the 1905 Jacobson v. Mass case, the court was clear that a PUBLIC BENEFIT was required for a vaccine to be mandated. Neither Pfizer nor Moderna have proved a disruption of transmission. In Jacobson v. Massachusetts, 197 U.S. 11 (1905), the court held that the context for their opinion rested on the following principle:
"This court has more than once recognized it as a fundamental principle that 'persons and property are subjected to all kinds of restraints and burdens in order to secure the general comfort, health, and prosperity of the state..."
The Moderna and Pfizer "alleged vaccine" trials have explicitly acknowledged that their gene therapy technology has no impact on viral infection or transmission whatsoever and merely conveys to the recipient the capacity to produce an S1 spike protein endogenously by the introduction of a synthetic mRNA sequence. Therefore, the basis for the Massachusetts statute and the Supreme Court's determination is moot in this case.
Further, the USPTO, in its REJECTION of Anthony Fauci's HIV vaccine made the following statement supporting their rejection of his bogus "invention"
Application/Control Number: 09/869,003 Page 5 Art Unit: 1648
These arguments are persuasive to the extent that an antigenic peptide stimulates an immune response that may produce antibodies that bind to a specific peptide or protein but is not persuasive in regards to a vaccine. The immune response produced by a vaccine must be more than merely some immune response but must be protective. As noted in the previous
Office Action, the art recognizes the term ~vaccine" to be a compound which prevents infection. Applicant has not demonstrated that the instantly claimed vaccine meets even the lower standard set forth in the specification, let alone the standard art definition, for being operative in this regards. Therefore, claims 5, 7, and 9 are not operative as an anti-HIV-1 vaccine and therefore lack patentable utility.
Indirectly, unlawfully and willfully provides or collects funds with the intention that such funds be used, or with the knowledge that such funds are to be used, in full or in part, in order to carry out-
(A) an act which constitutes an offense within the scope of a treaty specified in subsection (e)(7), as implemented by the United States, or
(B) any other act intended to cause death or serious bodily injury to a civilian, or to any other person not taking an active part in the hostilities in a situation of armed conflict, when the purpose of such act, by its nature or context, is to intimidate a population, or to compel a government or an international organization to do or to abstain from doing any act ....
By no later than April 11, 2005, Dr. Anthony Fauci was publicly acknowledging the association of SARS with bioterror potential. Leveraging the fear of the anthrax bioterrorism of 2001, he publicly celebrated the economic boon that domestic terror had directed towards his budget. He specifically stated that NIAID was actively funding research on a "SARS Chip" DNA microarray to rapidly detect SARS (something that was not made available during the current "pandemic") and two candidate vaccines focused on the SARS CoV spike protein.7 Led by three Chinese researchers under his employment- Zhi-yong Yang, Wing-pui Kong, and Yue Huang- Fauci had at least one DNA vaccine in animal trials by 2004.8 This team, part of the Vaccine Research Center at NIAID, was primarily focused on HIV vaccine development but was tasked to identify SARS vaccine candidates as well. Working in collaboration with Sanofi, Scripps Institute, Harvard, MIT and NIH, Dr. Fauci's decision to unilaterally promote vaccines as a primary intervention for several designated "infectious diseases" precluded proven therapies from being applied to the sick and dying.9
The CDC and NIAID led by Anthony Fauci entered into trade among States (including, but not limited to working with EcoHealth Alliance Inc.) and with foreign nations (specifically, the Wuhan Institute of Virology and the Chinese Academy of Sciences) through the 2014 et seq National Institutes of Health Grant R01AIl10964 to exploit their patent rights. This research was known to involve surface proteins in coronavirus that had the capacity to directly infect human respiratory systems. In flagrant violation of the NIH moratorium on gain of function research, NIAID and Ralph Baric persisted in working with chimeric coronavirus components specifically to amplify the pathogenicity of the biologic material.
By October 2013, the Wuhan Institute of Virology i coronavirus 51 spike protein was described in NIAID's funded work in China. This work involved NIAID, USAID, and Peter Daszak, the head of EcoHealth Alliance. This work, funded under R01AI079231, was pivotal in isolating and manipulating viral fragments selected from sites across China which contained high risk for severe human response.1°
By March 2015, both the virulence of the $1 spike protein and the ACE II receptor was known to present a considerable risk to human health. NIAID, EcoHealth Alliance and numerous researchers lamented the fact that the public was not sufficiently concerned about coronavirus to adequately fund their desired research.1~ Dr. Peter Daszak of EcoHealth Alliance offered the following assessment:
"Daszak reiterated that, until an infectious disease crisis is very real, present, and at an emergency threshold, it is often largely ignored. To sustain the funding base beyond the crisis, he said, we need to increase public understanding of the need for MCMs such as a pan-influenza or pan-coronavirus vaccine. A key driver is the media, and the economics follow the hype. We need to use that hype to our advantage to get to the real issues. Investors will respond if they see profit at the end of process, Daszak stated."12
Economics will follow the hype.
The CDC and NIAID entered into trade among States (including, but not limited to working with University of North Carolina, Chapel Hill) and with foreign nations (specifically, the Wuhan Institute of Virology and the Chinese Academy of
Sciences represented by Zheng-Li Shi) through U19AI109761 (Ralph S. Baric), U19AI107810 (Ralph S. Baric), and National Natural Science Foundation of China Award 81290341 (Zheng-Li Shi) et al. 2015-2016. These projects took place during
a time when the work being performed was prohibited by the United States National Institutes of Health.
The public was clearly advised of the dangers being presented by NIAID-funded research by 2015 and 2016 when the Wuhan Institute of Virology material was being manipulated at UNC in Ralph Baric's lab.
"The only impact of this work is the creation, in a lab, of a new, non-natural risk," agrees Richard Ebright, a molecular biologist and biodefence expert at Rutgers University in Piscataway, New Jersey. Both Ebright and Wain-Hobson are long-standing critics of gain-of-function research.
In their paper, the study authors also concede that funders may think twice about allowing such experiments in the future. "Scientific review panels may deem similar studies building chimeric viruses based on circulating strains too risky to pursue," they write, adding that discussion is needed as to "whether these types of chimeric virus studies warrant further investigation versus the inherent risks involved':
But Baric and others say the research did have benefits. The study findings "move this virus from a candidate emerging pathogen to a clear and present danger'; says Peter Daszak, who co-authored the 2013 paper. Daszak is president of the EcoHealth Alliance, an international network of scientists, headquartered in New York City, that samples viruses from animals and people in emerging-diseases hotspots across the globe.
Studies testing hybrid viruses in human cell culture and animal models are limited in what they can say about the threat posed by a wild virus, Daszak agrees. But he argues that they can help indicate which pathogens should be prioritized for further research atten tion."13
Knowing that the U.S. Department of Health and Human Services (through CDC, NIH, NIAID, and their funded laboratories and commercial partners) had patents on each proposed element of medical counter measures and their funding, Dr. Fauci, Dr. Gao (China CDC), and Dr. Elias (Bill and Melinda Gates Foundation) conspired to commit acts of terror on the global population - including the citizens of the United States - when, in September 2019, they published the following mandate:
"Countries, donors and multilateral institutions must be prepared for the worst. A rapidly spreading pandemic due to a lethal respiratory pathogen (whether naturally emergent or accidentally or deliberately released) poses additional preparedness requirements. Donors and multilateral institutions must ensure adequate investment in developing innovative vaccines and therapeutics, surge manufacturing capacity, broad-spectrum antivirals and appropriate non- pharmaceutical interventions. All countries must develop a system for immediately sharing genome sequences of any new pathogen for public health purposes along with the means to share limited medical countermeasures across countries.
Progress indicator(s) by September 2020
Donors and countries commit and identify timefinesfor: financing and development of a universal influenza vaccine, broad spectrum antivirals, and targeted therapeutics. WHO and its Member States develop options for standard procedures and timelines for sharing of sequence data, specimens, and medical countermeasures for pathogens other than influenza.
Donors, countries and multilateral institutions develop a multi-year plan and approach for strengthening R&D research capacity, in advance of and during an epidemic.
WHO, the United Nations Children's Fund, the International Federation of Red Cross and Red Crescent Societies, academic and other partners identify strategies for increasing capacity and integration of social science approaches and researchers across the entire preparedness/response continuum. ,14
As if to confirm the utility of the September 2029 demand for "financing and development of" vaccine and the fortuitous SARS CoV-2 alleged outbreak in December of 2029, Dr. Fauci began gloating that his fortunes for additional funding were likely changing for the better. In a February 2020 interview in STAT, he was quoted as follows:
""The emergence of the new virus is going to change that figure, likely considerably, Fauci said. "1 don't know how much it's going to be. But I think it's going to generate more sustained interest in coronaviruses because it's very clear that coronaviruses can do really interesting things.''
18 U.S.C. § 2331 §§ 802 -Acts of Domestic Terrorism resulting in death of
American Citizens
Section 802 of the USA PATRIOT Act (Pub. L. No. 107-52) expanded the definition of terrorism to cover "domestic," as opposed to international, terrorism. A person engages in domestic terrorism if they do an act "dangerous to human
life" that is a violation of the criminal laws of a state or the United States, if the act appears to be intended to: (i) intimidate or coerce a civilian population; (ii) influence the policy of a government by intimidation or coercion;
Dr. Anthony Fauci has intimidated and coerced a civilian population and sought to influence the policy of a government by intimidation and coercion.
With no corroboration, Dr. Anthony Fauci promoted16 Professor Neil Ferguson's computer simulation derived claims that,
"The world is facing the most serious public health crisis in generations. Here we provide concrete estimates of the scale of the threat countries now face.
"We use the latest estimates of severity to show that policy strategies which aim to mitigate the epidemic might halve deaths and reduce peak healthcare demand by two-thirds, but that this will not be enough to prevent health systems being overwhelmed. More intensive, and socially disruptive interventions will therefore be required to suppress transmission to low levels. It is likely such measures - most notably, large scale social distancing - will need to be in place for many months, perhaps until a vaccine becomes available." 17
Reporting to the President that as many as 2.2 million deaths may result from a pathogen that had not yet been isolated and could not be measured with any accuracy, Dr. Fauci intimidated and coerced the population and the government into reckless, untested, and harmful acts creating irreparable harm to lives and livelihoods.18 Neither the Imperial College nor the "independent" Institute for Health Metrics and Evaluation (principally funded by the Bill and Melinda Gates Foundation)19 had any evidence of success in estimating previous burdens from coronavirus but, without consultation or peer-review, Dr. Fauci adopted their terrifying estimates as the basis for interventions that are explicitly against medical advice.
The imposition of social distancing was based on computer simulation and environmental models with NO disease transmission evidence whatsoever.
The imposition of face mask wearing was directly against controlled clinical trial evidence and against the written policy in the Journal of the American Medical Association.
"Face masks should not be worn by healthy individuals to protect themselves from acquiring respiratory infection because there is no evidence to suggest that face masks worn by healthy individuals are effective in preventing people from becoming ill."2°
In both the Imperial College and the IHME simulations, quarantines were modeled for the sick, not the healthy.
Insisting on vaccines while blockading the emergency use of proven pharmaceutical interventions may have contributed to the death of many patients and otherwise healthy individuals.21
Using the power of NIAID during the alleged pandemic, Dr. Anthony Fauci actively suppressed proven medical countermeasures used by, and validated in scientific proceedings, that offered alternatives to the products funded by his conspiring entities for which he had provided direct funding and for whom he would receive tangible and intangible benefit.
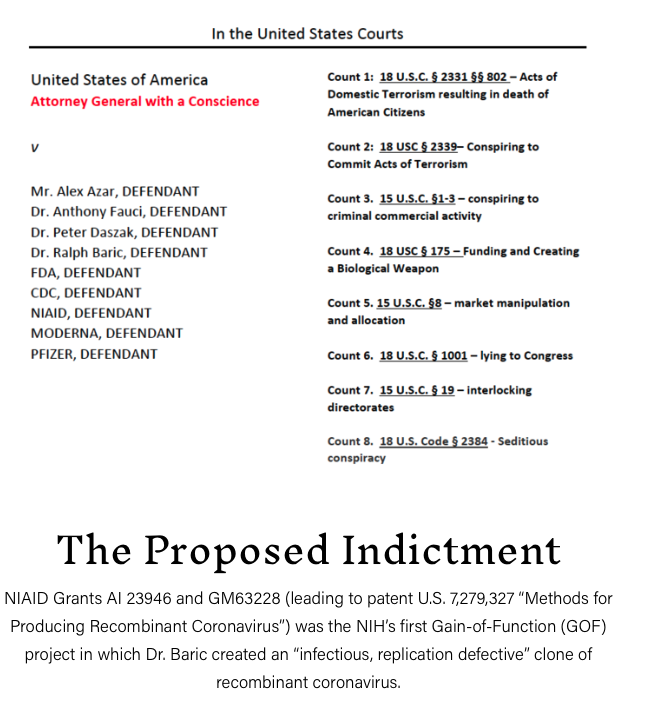
18 U.S.C. § tOOt - Lying to Congress
(a)Except as otherwise provided in this section, whoever, in any matter within the jurisdiction of the executive, legislative, or judicial branch of the Government of the United States, knowingly and willfully-
(Z) falsifies, conceals, or covers up by any trick, scheme, or device a material fact;
(2) makes any materially false, fictitious, or fraudulent statement or representation; or
(3) makes or uses any false writing or document knowing the same to contain any materially false, fictitious, or fraudulent statement or entry;
shall be fined under this title, imprisoned not more than 5 years or, if the offense involves international or domestic terrorism (as defined in section 2331), imprisoned not more than 8 years, or both. If the matter relates to an offense under chapter 109A, 109B, 110, or 117, or section 1591, then the term of imprisonment imposed under this section shall be not more than 8 years.
On October 22, 2020, the United States Government Accountability Office (GAG) published a report entitled:
BIOMEDICAL RESEARCH: NIH Should Publicly Report More Information about the Licensing of Its Intellectual Property.
In this document, the authors reported that the National Institutes of Health (NIH) received, "up to $2 billion in royalties from its contributions to 34 drugs sold from 1991-2019."22
A casual review of the NIH Office of Technology Transfer report of active licenses23 appears to conflict with the GAG report on several important facts. Conspicuously absent from the GAG report are over 30 patents associated with active compounds generating billions of dollars in revenue. Why would it be that the GAG and the NIH couldn't agree on something as simple as drugs generating income for NIH?
Since the passage of the Bayh Dole Act (Pub. L. 96-517, December 12, 1980), federally funded research has been an economic bonanza for U.S. universities, federal agencies, and their selected patronage. For the first decade following Bayh Dole, NIH funding doubled from $3.4 billion to $7.1 billion. A decade later, it doubled again to $15.6 billion. In the wake of September 2001, the National Institute for Allergy and Infectious Diseases (NIAID) saw its direct budget increase over 300% without accounting for DARPA funds of as much as $1.7 billion annually from 2005 forward. In 2020, NIH's budget was over $41 billion.
What has become of the $763 billion of taxpayer funds allocated to making America healthier since inventors have been commercially incentivized? Who has been enriched?
The answer, regrettably, is that no accountability exists to answer these questions.
The NIH is the named owner of at least 138 patents since 1980.
The United States Department of Health and Human Services is the named owner of at least 2,600 patents.
NIAID grants or collaboration have resulted in 2,655 patents and patent applications of which only 95 include an assignment to the Department of Health and Human Services as an owner. Most of these patents are assigned to universities thereby making the ultimate commercial beneficiaries entirely opaque. One of the largest holders is SIGA Technologies (NASDAQ: SIGA) who, while publicly reporting close affiliation with NIAID, is not referenced in the NIH GAG report. SIGA's CEG, Dr. Phillip L. Gomez spent 9 years at NIAID developing its vaccine program for HIV, SARS, Ebola, West Nile Virus, and Influenza before exiting to commercial ventures. While their technology is clearly derived from
NIAID science, the company reports revenue from NIAID but no royalty or commercial payments to NIH or any of its programs.
NIAID's Director, Dr. Anthony Fauci is listed as an inventor on 8 granted U.S. patents. None of them are reported in NIAID, NIH, or GAO reports of active licensing despite the fact that Dr. Fauci reportedly was compelled to get paid for his interleukin-2 "invention" - payments he reportedly donated to an unnamed charity.24
Of the 21 patents listed in the U.S. Food and Drug Administration's (FDA) Orange book itemized in the GAO report, none
of Dr. Anthony Fauci's patents are listed. Furthermore, none of the NIAID patents are listed despite clear evidence that Gilead Sciences and Janssen Pharmaceuticals (a division of Johnson & Johnson) have generated over $2 billion annually
from sales that were the direct result of NIAID funded science. Missing from the GAO report are 2 patents for Velclade® which has been generating sales in excess of $2.18 billion annually for several years. None of the patents for Yescarta®
are listed in the GAO report. None of the Lumoxiti® patents are listed in the GAO report. None of the Kepivance®
patents are listed in the GAO report. In violation of 37 USC §410.10 and 35 USC §202(a), over 13 of the 21 patents in the GAO report fail to disclose government interest despite being the direct result of NIH funding.
Dr. Anthony Fauci's Own Patent Track Record:
US Patent 6,190,656 and 6,548,055 Immunologic enhancement with intermittent interleukin-2 therapy
A method for activating a mammalian immune system entails a series of IL-2 administrations that are effected intermittently over an extended period. Each administration of IL-2 is sufficient to allow spontaneous DNA synthesis in peripheral blood or lymph node cells of the patient to increase and peak, and each subsequent administration follows the preceding administration in the series by a period of time that is sufficient to allow IL-2 receptor expression in peripheral or lymph node blood of the patient to increase, peak and then decrease to 50% of peak value. This intermittent IL-2 therapy can be combined with another therapy which targets a specific disease state, such as an anti- retroviral therapy comprising, for example, the administration of AZT, ddl or interferon alpha. In addition, IL-2 administration can be employed to facilitate in situ transduction of T cells in the context of gene therapy. By this approach the cells are first activated in viva via the aforementioned IL-2 therapy, and transduction then is effected by delivering a genetically engineered retroviral vector directly to the patient.
This application is a continuation of U.S. patent application Ser. No. 08/487,075, filed Jun. 7, 1995, now abandoned, which is a continuation in part of U.S. patent application Ser. No. 08/063,315, filed May 19, 1993, now issued as U.S. Pat.
No. 5,419,900, and U.S. patent application Ser. No. 08/452,440, filed May 26, 1995, now issued as U.S. Pat. No. 5,696,079, which is the National Stage filed under 35 USC 371 of PCT/US94/05397, filed May 19, 1994, the contents of which are incorporated herein by reference.
Filed May 19, 1993
Issued a Final Rejection January 20, 1998. Rejected after abandonment August 14, 1998 and April 12, 1999. Reduced and modified claims granted May 8, 2000.
This family of patents was the basis of Fauci's lie to the British Medical Journal in which he falsely stated:
"Dr Anthony Fauci told the BMJ that as a government employee he was required by law to put his name on the patent for
the development of interleukin 2 and was also required by law to receive part of the payment the government received for use of the patent. He said that he felt it was inappropiate (sic) to receive payment and donated the entire amount to charity."25
He was not "required by law" to commit fraud on the patent office and then get paid for it!
US Patent 6,911,527 HIV related peptides
This invention is the discovery of novel specific epitopes and antibodies associated with long term survival of HIV-1 infections. These epitopes and antibodies have use in preparing vaccines for preventing HIV-1 infection or for controlling progression to AIDS.
Filed May 6, 1999
Rejected as unpatentable January 22, 2003. Issued with a /inal rejection on July 15, 2004 after submitting reconsideration requests. Modi/ied and restricted daims allowed September 29, 2004.
US Patent 7,368,114 Fusion protein including of CD4
Novel recombinant polypeptides are disclosed herein that include a CD4 polypeptide ligated at its C-terminus with a portion of an immunoglobulin comprising a hinge region and a constant domain of a mammalian immunoglobulin heavy chain. The portion or the IgG is fused at its C-terminus with a polypeptide comprising a tailpiece from the C-terminus of the heavy chain of an IgA antibody ara tailpiece from a C-terminus of the heavy chain of an IgM antibody. Also disclosed herein are methods for using these CD4 fusion proteins.
Filed October 24, 2002
Rejected as unpatentable August 18, 2006. Paid appeal to overturn examiner's /indings February 15, 2007. Rejected again May 11, 2007. On October 10, 2007 applicants /urther narrowed the construction o/ what was dearly not a patent and the USPTO granted less than hal/the claims that had been sought in the original /iling.
US Patent 9,896,509, 9,193,790 and 9,441,041 Use of antagonists of the interaction between HIV GP120 and .alpha.4.beta.7 integrin
Methods are provided for the treatment of a HIV infection. The methods can include administering to a subject with an HIV infection a therapeutically effective amount of an agent that interferes with the interaction of gp120 and .alpha.4 integrin, such as a .alpha.4.beta.1 or .alpha.4.beta.7 integrin antagonist, thereby treating the HIV infection. In several examples, the .alpha.4 integrin antagonist is a monoclonal antibody that specifically binds to a .alpha.4, .beta.1 or .beta.7 integrin subunit or a cyclic hexapeptide with the amino acid sequence of CWLDVC. Methods are also provided to reduce HIV replication or infection. The methods include contacting a cell with an effective amount of an agent that interferes with the interaction of gp120 and .alpha.4 integrin, such as a .alpha.4.beta.1 or .alpha.4.beta.7 integrin antagonist. Moreover, methods are provided for determining if an agent is useful to treat HIV.
Rejected May 22, 2017 as Double Patenting. In their response, the applicants acknowledge the illegal act and seek only those components o/their application that extend beyond the li/e o/the issued patents. On October 11, 2017, the limited claims were issued.
A sample of the convoluted flow of funds that evades public disclosure.
U.S. Patent 8,999,351 was issued to Tekmira Pharmaceuticals Corporation in Burnaby, British Columbia. In their patent, they disclose that their research was supported by a grant from the National Institute of Allergy and Infectious Disease
(Grant HHSN266200600012C). Ironically, this $23 million grant was awarded in 2006 to Alnylam Pharmaceuticals, Inc., not to Tekmira.26 [CONT HERE]
No Matter How Much Death or Injury the Vax Causes and No Matter What the "Science Says" The Dependent Media Will Push the Vax: Media Hoaxed Sheeple Cause a Surge in Deadly Injections at CVS/Walgreens
/
DON’T BELIEVE THE HYPE AND DON’T BULLSHIT YOURSELF. THE DEPENDENT MEDIA ARE COMPLICIT IN CRIMES AGAINST HUMANITY. CONSTANT PARROTING OF SCIENCE-FREE MEDICINE is INTENDED TO coercE and intimidate obedient citizens into injecting themselves with deadly pathogens. NOTHING ANY OF THESE MOTHERFUCKING WHORES SAY SHOULD BE TAKEN AT FACE VALUE.
From [WSJ] The U.S. has plenty of Covid-19 vaccines but retail pharmacies are struggling to quickly administer them in some places.
Vaccine seekers in some states face waits of days or weeks for doses as local health officials hustle to improve access to meet surging demand. CVS Health Corp. , Walgreens Boots Alliance Inc. and Walmart Inc., which are facing staffing shortages, now say they may not be able to accommodate people without appointments.
Millions of Americans are newly eligible for booster shots, and federal health officials in November recommended the vaccine for use in children as young as 5 years old.
Media hyped concerns about the new Omicron variant also are driving more people to get vaccinated, health officials say. Omicron may be spreading quickly but it is producing no serious symptoms in those who are said to be “infected” with it. [MORE] In fact the The South African doctor who found "Omicron" says governments and media are over-reacting to a mild illness that appears to be like the common cold. [MORE]
An average of 1.4 million doses were administered daily in the U.S. in the week ended Thursday, a 22% increase from the previous week, which included Thanksgiving, according to the Centers for Disease Control and Prevention. [MORE]
From [UNZ] Question– Does the Covid-19 vaccine cause heart attacks?
Answer– It does, and researchers are closer to understanding the mechanism that triggers those events.
Question– How can I be sure you’re telling the truth?
Answer– Well, for starters, there’s a research paper that appeared recently in the prestigious Circulation magazine that draws the same conclusion. Here’s an excerpt from the paper:
“We conclude that the mRNA vacs dramatically increase inflammation on the endothelium (layer of cells lining the blood vessels) and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis (clotting), cardiomyopathy, (a group of diseases that affect the heart muscle) and other vascular events following vaccination.” (“Abstract 10712: Mrna COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: a Warning”, Circulation)
It’s actually quite rare for researchers to be so blunt in their analysis, but there it is in black and white. As you can see, they didn’t pull their punches. Here’s how Alex Berenson summed it up on his blogsite at Substack:
“A new study of 566 patients who received either the Pfizer or Moderna vaccines shows that signs of cardiovascular damage soared following the shots. The risk of heart attacks or other severe coronary problems more than doubled months after the vaccines were administered, based on changes in markers of inflammation and other cell damage. Patients had a 1 in 4 risk for severe problems after the vaccines, compared to 1 in 9 before. (“If you like heart problems, you’ll love the Pfizer and Moderna Covid vaccines”, Alex Berenson, Substack)
“Doubled”? “The risk of heart attacks.. more than doubled” after vaccination?
Apparently, so. No wonder cardiologist Dr. Aseem Malhotra is so flabbergasted. Here’s what he said in a recent interview:
“Extraordinary, disturbing and upsetting. We now have evidence of a plausible biological mechanism of how mRNA vaccine may be contributing to increased cardiac events. The abstract is published in the highest impact cardiology journal so we must take these findings very seriously.”
Indeed, we must, but our public health experts continue to pretend that nothing has changed, even though more and more professionals continue to speak out. Here’s Malhotra again:
“I have alot of interaction with the cardiology community across the UK, and anecdotally, I have been told by colleagues that they are seeing younger and younger people coming in with heart attacks…. Now since July, there’s been at least 10,000 non-covid deaths, and most of those have been driven by circulatory disease, in other words, heart attack and stroke. And there’s been a 30% increase in deaths at home, often because of cardiac arrest…. (So) The signal is quite strong… This needs to be investigated… And I think it is high-time that policymakers around the world put an end to the mandates, because –if this signal is correct– then history will not be on their side and the public will not forgive them for it.” (Dr Aseem Malhotra reveals increase in risk of heart attack following the mRNA COVID vaccine, Bitchute, Minute-1:35) [MORE]
Dr Peter McCullough: So-Called COVID "Vaccines" Are Grossly Unsafe and Lethal
/From [NN] Dr. Peter McCullough warned that diseases caused by Wuhan coronavirus (COVID-19) vaccines are a “leading public health threat.” Instead of protecting people from the disease, COVID-19 vaccines are causing injuries and deaths.
McCullough is an internist, cardiologist and epidemiologist who practices medicine in Dallas. He helps patients dealing with various cardiovascular complications caused by the coronavirus (SARS-CoV-2) and the COVID-19 vaccines.
In a recent episode of his podcast “The McCullough Report,” he interviewed Dr. Bruce Patterson to discuss COVID vaccines and spike proteins.
According to Patterson, the spike protein from SARS-CoV-2 may be harmful and inflammatory on its own. The spike protein can also linger in the human body for as long as 15 months after a severe infection. (Related: Army surgeon warned that pilots could die in midair from COVID vaccine injuries… but was ignored.)
The mRNA injections instruct your body to make a similar version of this virus’s spike protein, which can start to accumulate in tissues throughout the body. The spike proteins created because of the vaccines are very likely behind the reported cases of adverse reactions in vaccinated individuals.
McCullough explained that as the pandemic ebbs, the public “can expect to learn and hear more about how the COVID-19 vaccines – which are now administered by mandate and in some countries by force – grow in strength as the leading public health threat and become significant determinants of a whole new class of illnesses leading to disability, hospitalization and death.”
During the wait for long-term data on coronavirus vaccines, the virus continues to mutate, which spells trouble for mass vaccination efforts. Reports say that the pandemic is nowhere near the end, especially since new variants continue to be reported.
After Thanksgiving in the U.S., mainstream media started spreading fear and panic among citizens about the latest coronavirus variant called omicron. Allegedly, omicron is more transmissible, but this doesn’t necessarily mean it’s more dangerous than current COVID-19 variants.
Dr. Anthony Fauci, President Joe Biden’s chief medical advisor, predicted that the omicron variant will spread “all over.” Experts have yet to determine if current coronavirus vaccines are effective against the new variant.
According to data from the Centers for Disease Control and Prevention (CDC), coronavirus vaccines aren’t 100 percent effective against existing variants of the virus for many individuals. This suggests that mRNA vaccines won’t be as effective against the omicron variant.

Vaccine expert: Mass vaccination during pandemic is dangerous
Virus mutations are natural. The problem is, viruses will evolve much faster if there is a lot of pressure on them to do so – such as when a worldwide vaccination program is enforced during an “ongoing and rapidly evolving pandemic.”
This phenomenon was described in detail by Dr. Geert Vanden Bossche, a Belgian virologist, vaccine expert and former employee of The Bill & Melinda Gates Foundation. He uploaded on his website an open letter calling on the World Health Organization(WHO) to immediately halt all coronavirus (COVID-19) mass vaccinations.
“This type of prophylactic vaccines is completely inappropriate, and even highly dangerous, when used in mass vaccination campaigns during a viral pandemic,” he wrote.
A prophylactic or preventative vaccine involves introducing antigens into a person’s body. The goal is that the individual’s immune system will create antibodies for those antigens, and become immune to the associated illness.
According to Vanden Bossche, the mass vaccination drives are “likely to further enhance adaptive immune escape as none of the current vaccines will prevent replication or transmission of viral variants.” Immune escape is a term used to describe when the host is no longer able to recognize and counter a pathogen, such as a relevant variant or mutant of SARS-CoV-2.
Bossche concluded his letter by encouraging the WHO and all stakeholders to take immediate action and address this public health threat of international concern.
Visit VaccineInjuryNews.com for more news on vaccine-related injuries and deaths.
A Tweet Referenced an American Heart Association Science Article that said 'mRNA Vaccines Increase the Risk of Heart Damage,' So Twitter Flagged It
/
From [HERE] New research from the American Heart Association (AHA) has been censored on Twitter because it exposes the serious health risks associated with Wuhan coronavirus (Covid-19) “vaccines.”
A link to this study that was tweeted by someone named Marina Medvin now brings up a bizarre and false prompt from Twitter that reads: “Warning: this link may be unsafe.”
Users are then urged to click the “Back to previous page” button to avoid accessing the article, though there is also a tiny link at the bottom that says, “Ignore this warning and continue.”
The study was published in the AHA journal Circulation, and it clearly explains how mRNA (messenger RNA) Chinese Virus injections “dramatically increase endothelial inflammatory markers,” thus increasing the risk of acute coronary syndrome (ACS).
Mind you, this is an official study published by the AHA, which if it supported the jab narrative would be perfectly fine with Twitter’s censors. However, because it defies fake government “doctor” Tony Fauci’s guidelines for the plandemic, the study is no longer allowed on Twitter.
“The Journal of the American Heart Association puts out a study warning of the impact of mRNA Covid vaccines on the heart,” tweeted someone else in disgust. “Twitter reflexively applies a warning that the site may be unsafe. THE F’ING AMERICAN HEART ASSOCIATION?!?”
AHA issues “expression of concern” about study over “several typographical errors”
When this writer first reported on the Circulation study, it was observed that there were a few misspellings and grammatical errors, which the AHA apparently noticed as well.
Because of these, the AHA issued an “expression of concern” about the study highlighting these “several typographical errors.” The organization also now claims that there is “no data in the abstract regarding myocardial T-cell infiltration” or “statistical analyses for significant provided.”
Twitter jumped all over this and took the opportunity to further claim erroneously that the study itself is “potentially spammy or unsafe” and could contain “malicious links that could steal personal information or harm electronic devices.”
Twitter further insisted that the study could “mislead people or disrupt their experience” because it supposedly contains “violent or misleading content that could lead to real-world harm.”
“[C]ertain categories of content that, if posted directly to Twitter, are a violation of the Twitter Rules” was also slapped across the study link to try to deter users from viewing it.
Which of these Twitter believes apply to the Circulation study remains unclear, though it is possible that employees at the social media giant consider all of them to be applicable to its contents.
“A warning by Twitter is usually a warning to us to take heed of what has been tweeted,” noted one commenter at Zero Hedge.
“A warning by Twitter is usually a warning to just get the **** off Twitter,” responded another.
Another joked that surely Twitter must know more than the AHA about cardiology, seeing as how it is the self-aggrandizing expert in everything.
“The question that people should be asking about this and similar acts of blatant censorship by Twitter is why would it be necessary to censor medical facts which conflict with the official narrative IF said narrative holds water?” this same commenter added.
Yet another pointed out that the so-called “vaccines” for the Fauci Flu are clearly far more dangerous than any alleged virus, assuming one even exists.
“If they say that it is true, it is probably false,” wrote another about Twitter’s “standards.” “If they say that it is false, then it is probably true.”
These “variants" are Produced in Response to the Vax. In other words Government and Big Pharma have Unleashed an ever changing virus upon the world. The only hope is to Immediately Stop All Injections
/From [HERE] These “mutant strains” or variants are produced in response to the Covid vaccine. In other words, Fauci, Big Pharma, the medical establishment, and dumbshit politicians have unleashed an ever changing virus upon the world. The only hope is to immediately stop all Covid vaccination.
The Covid vaccinated are a grave threat to the unvaccinated, not only because the vaccinated “shed” the virus, thus spreading the virus to others, but also because the vaccine enables the virus to mutate in order to escape an immune response. The immunity the mutated variant of the virus achieves from the vaccine also gives the virus protection against the innate human immune system. In other words, people who have not damaged their innate immune system by taking the vaccine could now be confronted with a variant that their immune system is less able to repel.
What Fauci has done by financing the creation of the Covid-19 virus and by walking Big Pharma’s “vaccine” through the emergency use process is to create a Frankenstein virus capable of escaping immune responses.
How bad for humanity this turns out to be remains to be seen. What we do know is the more people are vaccinated, the worse it will be. All Covid vaccination should be stopped immediately before damage to the immune system makes more people susceptible to illnesses and death.
If we add in to the equation the known facts that the vaccine itself causes injurious and lethal side-effects and damages the innate immune system, making the vaccinated more susceptible to all other viruses and diseases, the Covid vaccine is a threat to human life on the level of thermonuclear weapons.
To attribute the Covid “vaccine” to a mere mistake of the medical establishment seems farfetched. Covid-19 was not a threat that justified the risk of a gene-altering experimental vaccine being used on the mass of humanity. It really does look like a program to reduce the human population.
If the new variants prove to be more infectious and more deadly, what will an incompetent or corrupt medical establishment blame them on? Will the unvaccinated continue to be the scapegoat? Will Australia’s concentration camps spread throughout the world? Will a new virus be released to blame for the failure of the mRNA vaccine? Is a release of smallpox in our future? https://www.paulcraigroberts.org/2021/11/23/is-a-smallpox-plague-being-organized-for-us/
We have reached the point where it is clear that we can have zero confidence in the medical establishment, an establishment that intentionally withholds known safe and effective treatments from dying patients in order to maximize its revenues– https://childrenshealthdefense.org/defender/paul-marik-lawsuit-hospital-remdesivir-ban-life-saving-drugs/
Judging by the high rates of vaccination in the Western countries, majorities of populations have been brainwashed and see the deadly vaccination protocol as protection. The media has systematically misrepresented the Covid threat from the beginning and is now too responsible for scaring mass numbers of people into injury and death to own up to the facts. The media will continue to lie in order to protect itself and the medical establishment.
It seems the governments of the “free world” will not be content until 100% vaccination rates are enforced either via Austria’s policy of confining the entire population to house arrest or Australia’s policy of herding people into concentration camps.
Court Docs Reveal Phizer/FDA Knew the Vax was Killing and Injuring People at a High Rate in Early 2021. Phizer Hid Info Essential to Informed Consent and Falsely Claimed Vax is “safe and effective”
/
From [AARON SIRI] and (Natural News) and [HERE] Two months and one day after it was sued, and close to 3 months since it licensed Pfizer’s Covid-19 vaccine, the FDA released the first round of documents it reviewed before licensing this product. The production consisted of 91 pdf pages, one xpt file, and one txt file. You can download them here or https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf or https://www.naturalnews.com/files/536-postmarketing-experience.pdf
Said documents that show Pfizer and the FDA knew in early 2021 that pfizer’s mRNA vaccines were killing people and causing injury.
Previously, the FDA repeatedly promised “full transparency” with regard to Covid-19 vaccines, including reaffirming “the FDA’s commitment to transparency” when licensing Pfizer’s COVID-19 vaccine.
Additionally, under Title 21, sub-chapter F of the FDA’s own regulations, the agency “is to make ‘immediately available’ all documents underlying licensure of a vaccine.”
In August and immediately following approval of the vaccine, more than 30 academics, professors, and scientists from the most prestigious universities requested the data and information submitted to the FDA by Pfizer to license its COVID-19 vaccine.
The FDA’s response? It produced nothing. So, in September,a lawsuit was filed against the FDA on behalf of this group to demand this information.
The FDA then asked a federal judge to make the public wait until the year 2076 to disclose all of the data and information it relied upon to license Pfizer’s COVID-19 vaccine. That is not a typo. It requested 55 years to produce critical information on the vaccine and otherwise withhold it from the public.
A federal judge in Texas denied the request and ordered that the 329,000 documents from Pfizer be released at a rate of 500-page-per-month, albeit with redactions. Said process of court ordered transparency will occur at a snail’s pace. Meanwhile, people’s lives are being ruined over vaccine injury and vaccine coercion, as the data is slowly released, the truth painstakingly exposed.
The documents reveal the FDA tried to conceal widespread vaccine injury and death from Pfizer’s mRNA vaccine.
In the first three months of the vaccine’s rollout, there were voluntary reports of 1,223 deaths and over 42,000 adverse reports spanning a total of 158,893 adverse reactions. One of every 37 reports was DEATH! This data was only from vaccines that were administered between December 1st to February 28. The data was collected from the United States, Germany, the United Kingdom, Italy, France, Spain and a host of other nations.
Pfizer knew that their vaccine was killing and injuring people at rates never seen before in the history of vaccinology, yet the FDA helped the fully-indemnified pharmaceutical cartel conceal this information and achieve full licensure with their Comirnaty mRNA vaccine. The two entities conspired to withhold critical, life-and-death medical information that is essential for informed consent, and continue to allow dangerous inoculations to cause unprecedented levels of nervous system disorders, cardiovascular events and autoimmune reactions. It should have been pulled from the market.
The true number of vaccine injuries and deaths that occurred in this three-month time span and thereafter is unknown. Nevertheless, even these numbers — already quite shocking, given the FDA’s insistence that mRNA vaccines are “safe and effective” — barely scratch the surface of the damage and deaths caused by these vaccines. “Reports are submitted voluntarily, and the magnitude of underreporting is unknown,” says Pfizer on page 5.
In the documents, Pfizer admitted there was no data on the vaccine’s effectiveness or evidence of safety for children and pregnant and lactating women. Nevertheless the government pushed the vaccine for pregnant women and children anyway. According to the documents, the FDA also knew in advance that the vaccine could sicken and kill patients who were later infected with covid — in what was referred to as “Vaccine-Associated Enhanced Disease, including Vaccine-associated Enhanced Respiratory Disease.”
Three times as many women damaged, compared to men
Shockingly, the document reveals that more than three times as many women were damaged by the Pfizer vaccine, compared to men. There were 29,914 adverse events recorded in women, with just 9,182 recorded in men. It is not known whether the same number of men and women took the vaccine, but this number exposes the very real possibility of a gender-specific vaccine damage risk that the FDA went to great lengths to cover up.
Anecdotally, most of the neurological damage we’ve seen in people who have been damaged by the vaccine — convulsions, numbness, pain, etc. — has been depicted in women, not men. It looks like the FDA knows the mRNA vaccine exhibits a disproportionate, gender-specific damage profile that also affects women in terms of spontaneous abortions (also covered in the report).
Pfizer told the FDA its mRNA covid vaccines can cause “enhanced disease” by making covid worse
Also to the shock of many observers who are just now digging into this smoking gun document, Pfizer told the FDA under “Safety concerns” (section 3.1.2) that its mRNA injection could cause, “Vaccine-Associated Enhanced Disease (VAED), including Vaccine-associated Enhanced Respiratory Disease (VAERD).”
This means the FDA knew the vaccine could sicken and kill patients who were later infected with covid.
Under the label of “missing information,” Pfizer also told the FDA that it has no information about “Use in Pregnancy and lactation” nor covering “Use in Paediatric Individuals < 12 Years of Age.”
“Vaccine Effectiveness” was also listead as “Missing information” by Pfizer.
In other words, Pfizer told the FDA its vaccines could kill people and that it had no information about vaccine effectiveness, yet the FDA fraudulently pushed the vaccine as “safe and effective” anyway. Pfizer even told the FDA that it had no safety information about use in pregnant women, yet the FDA (and Fauci, the CDC, etc.) all pushed the vaccine for pregnant women, despite the utter lack of safety information.
Based on this document, it appears that the FDA itself has been neck-deep in a criminal conspiracy to hide the truth about vaccine injuries and deaths while granting usage approvals to the very same corporations that openly told the FDA its products were killing people.
Note, too, that the entire corporate media complex has lied from day one, falsely claiming the vaccine has killed no one. They are, of course, complicit in this vaccine holocaust.
Spontaneous abortions, neonatal death and other effects on pregnant women
In the section labeled, “Use in Pregnancy and lactation,” the report discusses reports of the mRNA vaccine being linked to:
spontaneous abortion (23), outcome pending (5), premature birth with neonatal death, spontaneous abortion with intrauterine death (2 each), spontaneous abortion with neonatal death, and normal outcome (1 each).
Notice that “spontaneous abortion” represents by far the highest number in these reports. In other words, the FDA knew this vaccine would kill unborn babies, but they pushed it on pregnant women anyway.
All mRNA vaccines must be immediately halted, and FDA bureaucrats must be indicted and arrested
This confidential document — just the first of thousands yet to be released — reveals two critical things:
1) The FDA committed criminal fraud and misrepresentation in approving mRNA vaccines as “safe and effective.” This means top FDA decision makers must now face arrest and criminal prosecution.
2) The mRNA vaccine was known by Pfizer to be deadly even in its first three months of emergency use. This means Pfizer is also complicit in the continued deaths of innocent victims, as Pfizer itself should have pulled its deadly vaccine and halted all sales and distribution.
The definition of a “vaccine” had to be completely changed in order to market and license these new mRNA injections. The clinical trials did not use proper diagnostic standards, did not study viral transmission, all-cause mortality, nor compare rates of severe illness. The process also ignored the myriad of health issues imparted by the vaccines, some of which are deliberately life threatening. The clinical trials relied on positive PCR testing rates (that have been proven fraudulent) and non-specific symptoms of mild illness in a small time period. This is how the vaccine makers came up with their flimsy vaccine efficacy rates, which have fallen into negative territory, when real world vaccine effectiveness is configured.