By [Suzanne Burdick, Ph.D.] A new analysis of Pfizer and Moderna COVID-19 vaccine trial data shows the risk of serious injury following the vaccine is greater than the reduction in COVID-19 hospitalizations, according to a study posted June 23 on Social Science Research Network.
“Combining the trials, there was a 43% increased risk of serious adverse events of special interest and an absolute risk increase of 12.5 serious adverse events of special interest per 10,000 vaccinated participants,” the authors of the pre-print paper wrote.
Based on their findings, the authors called for a harm-benefit analysis of COVID-19 vaccines.
The researchers — among them Peter Doshi, Ph.D., senior editor at The BMJ and associate professor of pharmaceutical health services research at the University of Maryland School of Pharmacy — concluded:
“A systematic review and meta-analysis using individual participant data should be undertaken to address questions of harm-benefit in various demographic subgroups. Full transparency of the COVID-19 vaccine clinical trial data is needed to properly evaluate these questions. Unfortunately, well over a year after widespread use of COVID-19 vaccines, participant-level data remain inaccessible.”
Doshi leads the Restoring Invisible & Abandoned Trials (RIAT) initiative, which seeks to ensure clinical trial publications are accurate and complete, and data are publicly available.
The study’s other authors are:
Robert Kaplan, Ph.D., who leads Stanford University’s Clinical Excellence Research Center and previously led the behavioral and social sciences programs at the National Institutes of Health and served as the chief science officer at the U.S. Agency for Health Care Research and Quality.
Dr. Patrick Whelan, M.D., Ph.D., associate clinical professor of pediatrics in the division of rheumatology at the University of California at Los Angeles (UCLA).
Sander Greenland, Ph.D., professor emeritus of epidemiology and statistics at UCLA who served as an advisor for the World Health Organization (WHO), the U.S. Food and Drug Administration (FDA), the Environmental Protection Agency, the Centers for Disease Control and Prevention and the National Academy of Sciences.
Mark Jones, Ph.D., associate professor of health sciences and medicine at the Institute for Evidence-Based Healthcare, as well as a biostatistician at Bond University in Robina, Australia.
Juan Erviti, Ph.D. Pharm. D., qualified hospital pharmacist at Navarre Health Service, Spain.
Dr. Joseph Fraiman, emergency medicine doctor at Louisiana State University’s Lallie Kemp Regional Medical Center.
“This important study uses actual Pfizer and Moderna clinical trial data to show that the risks of serious adverse events outweigh the benefits of these vaccines against COVID-19 hospitalization,” said Brian Hooker, Ph.D., Children’s Health Defense chief scientific officer and associate professor of biology at Simpson University in Redding, California where he specializes in microbiology and biotechnology.
“The public, and public health officials, need to immediately consider the implications of these study results,” Hooker added.
What the researchers did, and why
The researchers analyzed data from the clinical trials the FDA used as the basis for granting Emergency Use Authorization of the Pfizer and Moderna vaccines “to investigate the association between FDA-authorized mRNA COVID-19 vaccines and serious adverse events identified by the Brighton Collaboration.”
According to the researchers, the Brighton Collaboration in March 2020 created and later updated a priority list of “potential adverse events of special interest relevant to COVID-19 vaccine trials” in collaboration with the Coalition for Epidemic Preparedness Innovations partnership, Safety Platform for Emergency Vaccines.
The priority list identified serious health events as being “adverse events of special interest for safety monitoring” (AESIs) if they met one or more of the following criteria:
Known association with immunization or a specific vaccine platform.
Occurrence during wild-type disease as a result of viral replication and/or immunopathogenesis.
Theoretical association based on animal models.
The AESIs noted on this list included serious adverse events (SAEs) of the following types: cardiac, dermatologic, endocrine, gastrointestinal, hematologic, liver, kidney, multisystem inflammatory syndromes, musculoskeletal, neurologic, ocular, respiratory and pregnancy.
The WHO’s Global Advisory Committee on Vaccine Safety endorsed the list as a safety monitoring tool and recommended AESIs be reported based on the list — yet no research using the list was conducted on randomized trial data to determine the association between vaccination and the occurrence of AESIs, according to the study authors.
For this reason, the authors of the study conducted an analysis of SAEs reported in the placebo-controlled, Phase 3 randomized clinical trials of the Pfizer and Moderna mRNA COVID-19 vaccines (NCT04368728 and NCT04470427).
How they conducted the analysis
First, the team searched Pfizer and Moderna trial data on the FDA and Health Canada websites to locate SAE results tables for the trials.
Following regulatory norms, the two pharmaceutical companies used nearly identical definitions for what constituted a “serious” adverse event by deeming any adverse event to be an SAE if it resulted in any of the following conditions:
Death
Life-threatening at the time of the event
Inpatient hospitalization or prolongation of existing hospitalization
Persistent or significant disability/incapacity
A congenital anomaly/birth defect
Medically important event, based on medical judgment
Although Pfizer and Moderna were expected to follow participants for two years, within weeks of the FDA granting EUA of the vaccines, “the sponsors began a process of unblinding all participants who elected to be unblinded,” the authors said.
Additionally, participants who initially received the placebo were offered the vaccine.
“These self-selection processes may have introduced nonrandom differences between the vaccine and unvaccinated participants,” wrote the authors, “thus rendering the post-authorization data less reliable.”
To “preserve randomization,” the researchers used “the interim datasets that were the basis for emergency authorization in December 2020, approximately 4 months after trials commenced.”
Next, for each of these dataset trials, the researchers prepared blinded SAE tables — showing types of SAEs but not showing results data.
Then, two clinical reviewers used the tables to independently judge whether each SAE was an AESI.
Using statistical analyses, the team then calculated risk ratios and risk differences between the vaccine and placebo groups for the incidence of SAEs.
Finally, the researchers used a simple harm-benefit framework to place their results in context by comparing the risks of excess AESIs against reductions in serious complications of COVID-19.
What the results showed
The Pfizer trial reported a “36% higher risk of [SAEs] unrelated to COVID-19 in
175 vaccinated participants” compared with placebo recipients, the study’s authors reported.
“The Moderna trial reported a 5% higher risk of SAEs unrelated to COVID-19 in vaccinated individuals compared to those receiving placebo,” they wrote.
The researchers’ blind and independent review determined the majority of SAEs were AESIs — meaning most of these events were the type known to be of particular safety concern related to the COVID-19 vaccine.
The researchers’ findings contrast with Pfizer’s previous claim that nearly all SAEs during the vaccine trials were “not related” to the vaccine.
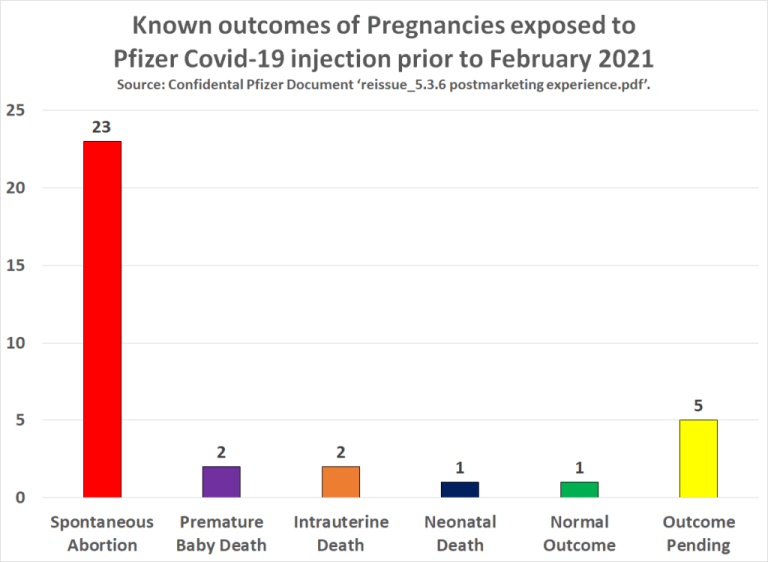
As The Defender reported, Pfizer-BioNTech COVID-19 vaccine documents released June 1 by the FDA revealed numerous instances of participants who sustained severe adverse events during Phase 3 trials.
Some of these participants withdrew from the trials, some were dropped and some died.
According to the study:
“In the Moderna trial, the excess risk of serious AESIs (15.1 per 10,000 participants) surpassed the risk reduction for COVID-19 hospitalization relative to the placebo group (6.4 per 10,000).
“In the Pfizer trial, the excess risk of serious AESIs (10.1 per 10,000) surpassed the risk reduction for COVID-19 hospitalization relative to the placebo group (2.3 per 10,000 participants).”
The authors noted limitations of their study, such as that their analysis used an existing dataset rather than recent data.
However, they noted, “Our analysis has an advantage over postmarketing observational studies in that the data are from blinded, placebo-controlled randomized trials vetted by the FDA, and uses the Brighton Collaboration AESI list, which was pre-specified, endorsed by WHO, and established well before the availability of the clinical trial results, and designed for use in COVID-19 vaccine trials.”
They also noted their results showing a heightened risk of AESIs in the vaccine group represented an average across the group.
“SAEs may not be distributed equally across the demographic subgroups enrolled in the trial, and the risks may be substantially less in some groups compared to others.”
“Knowing the actual demographics of those who experienced an increase in AESI in the vaccine group is necessary for a proper harm-benefits analysis,” they added