Funeral Home Stocks Surge, Death and Disability Payouts Soar
/STORY AT-A-GLANCE
Business is booming at funeral homes across the U.S. as death rates creep up, particularly among young, working-age individuals
Ex-Blackrock fund manager Ed Dowd has been analyzing data about mortality rates before and after COVID-19 shots became widespread, and found that death rates worsened in 2021 — after the shots became prevalent — compared to 2020
Insurance companies are seeing increases in payouts for death and disability; Lincoln National stated death claims have increased 13.7% year over year and 54% in quarter 4 compared to 2019
Scott Davison, the CEO of insurance company OneAmerica, reported the death rate for 18- to 64-year-olds has risen 40% compared to before the pandemic
A study by Dr. Peter McCullough and colleagues suggests people who’ve received COVID-19 shots may have damage to their innate immune system that’s leading to a form of acquired immunodeficiency syndrome
From [MERCOLA PDF] Business is booming at funeral homes across the U.S., as death rates creep up, particularly among young, working-age individuals.1 Ex-Blackrock fund manager Ed Dowd has been analyzing data about mortality rates before and after COVID-19 shots became widespread, and found that death rates worsened in 2021 — after the shots became prevalent — compared to 2020.
As reported by Zero Hedge, Dowd pointed out “a spike in mortality among younger, working-age individuals coincided with vaccine mandates. The spike in younger deaths peaked in Q3 2021 when COVID deaths were extremely low (but rising into the end of September).”2
Dowd also reported data from public funeral home company Carriage Services, which announced a 28% increase in September 2021 compared to September 2020, while August had a 13% increase. He tweeted:3,4
“Business has been quite good since the introduction of the vaccines & the stock was up 106% in 2021. Curious no? Guys this is shocking as 89% of Funeral homes are private in US. We are seeing the tip of the iceberg.”
Life Insurance Payouts on the Rise
Insurance companies are also seeing increases in payouts for death and disability. Dowd tweeted February 1, 2022, that financial insurance company Unum reported a 9% increase in their benefit ratio (payouts versus premiums) in their life segment.5 Dowd tweeted:6
“In 2021 they saw a 17.4% increase vs 2020. This is higher than the 13.3% increase vs 2019. So the higher payouts in 21 are occurring with a miracle vaccine & less virulent strains … In 2019 the unit had $266 million profit, last year a profit of $82 million & this year a loss of -$192 million. A swing of $458 million lower over 2 years. Important to remember these are employed working age folks.”
Scott Davison, the CEO of Indiana-based insurance company OneAmerica, also reported disturbing statistics — the death rate for 18- to 64-year-olds has risen 40% compared to before the pandemic.7
"We are seeing, right now, the highest death rates we have seen in the history of this business – not just at OneAmerica," Davison said, adding, “Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic. So 40% is just unheard of.” Further, most of the deaths are not due to COVID-19. He said:8
"What the data is showing to us is that the deaths that are being reported as COVID deaths greatly understate the actual death losses among working-age people from the pandemic. It may not all be COVID on their death certificate, but deaths are up just huge, huge numbers."
Disability Claims and Hospital Death Rates Rise
Disability claims, initially short-term claims and now long-term claims, have also seen an “uptick.” At a news conference where Davison spoke, Brian Tabor, president of the Indiana Hospital Association, confirmed that hospitals are also seeing widespread ill health and rising death rates. Zero Hedge reported:9
“Brian Tabor, the president of the Indiana Hospital Association, said that hospitals across the state are being flooded with patients ‘with many different conditions,’ saying ‘unfortunately, the average Hoosiers’ health has declined during the pandemic.’
In a follow-up call, he said he did not have a breakdown showing why so many people in the state are being hospitalized — for what conditions or ailments. But he said the extraordinarily high death rate quoted by Davison matched what hospitals in the state are seeing. ‘What it confirmed for me is it bore out what we're seeing on the front end ...’ he said.”
Other insurance companies citing higher mortality rates include Hartford Insurance Group, which announced mortality increased 32% from 2019 and 20% from 2020 prior to the shots. Lincoln National also stated death claims have increased 13.7% year over year and 54% in quarter 4 compared to 2019.10 Dowd tweeted:11
“Randy Frietag CFO just explained that in 2021 the share of young people dying from covid doubled in the back half of the year & that's driven the result for Lincoln & its peers. He cited 40% in 3Q and 35% in 4Q were below the age of 65 … Mandates are killing folks … This shouldn’t be happening with miracle vaccines in a working age population period and a mild Omicron.”
As ZeroHedge noted, what we need to know from the insurance companies is what the leading causes of death were for 2020 and 2021, as well as how many received COVID-19 shots among those who died.
It continued, “Reinsurance Group of America, for example, reported a profit in Q4 2020 when the most of the population was unvaccinated and amid a deadlier strain of Covid-19, yet they registered a loss in Q4 2021 with more than 60% of the country fully vaccinated (and around 75% who have received at least one dose).”12
In other words, they paid out more in death and disability benefits in late 2021, after the shots became widespread, then they did at the peak of the pandemic, when no shots (or only a small number) had been issued.
Deaths Keep Rising Despite Mass Injection Campaign
Around the globe, it’s become clear that excess deaths continue to explode, despite the mass injection campaign that was supposed to save us. In the week ending November 12, 2021, the U.K. reported 2,047 more deaths than occurred during the same period between 2015 and 2019.
However, COVID-19 cannot be entirely to blame, as it was listed on the death certificates for only 1,197 people.13 Further, since July, non-COVID deaths in the U.K. have been higher than the weekly average in the five years prior to the pandemic.
Heart disease and strokes appear to be behind many of the excess deaths, with Financial Times reporting, “The new phase of excess deaths raises the possibility that since the summer more people have been losing their lives as a result of strains on the NHS or lack of early diagnosis of serious illness …”14
On Twitter, Silicon Valley software engineer Ben M. (@USMortality) similarly revealed that in a 13-week period alone, about 107,700 seniors died above the normal rate, despite a 98.7% vaccination rate.15 In another example, he used data from the U.S. Centers for Disease Control and Prevention, census.gov and his own calculations to show excess deaths rising in Vermont even as the majority of adults have been injected.
“Vermont had 71% of their entire population vaccinated by June 1, 2021,” he tweeted. “That’s 83% of their adult population, yet they are seeing the most excess deaths now since the pandemic!”16
An investigation by The Exposé, using official data from NHS and the U.K.’s Office for National Statistics (ONS), also found that deaths among teenagers increased 47% since they started getting COVID-19 shots.17 Not only that, but deaths from COVID-19 also went up among 15- to 19-year-olds after the shots were rolled out for this age group.
COVID-19 Shots Causing Acquired Immunodeficiency Syndrome
A study by board-certified internist and cardiologist, and editor of two medical journals, Dr. Peter McCullough and colleagues suggests people who’ve received COVID-19 shots may have damage to their innate immune system that’s leading to a form of acquired immunodeficiency syndrome.18
The mRNA COVID-19 shots use genetically modified mRNA encoding spike proteins. This results in mRNA being hidden from cellular defenses, “promote[s] a longer biological half-life for the proteins, and provoke[s] higher overall spike protein production,” the study suggests.19
The researchers state that experimental and observational evidence show that the human immune response to COVID-19 shots is very different than the response induced by exposure to SARS-CoV-2:20
“[T]he genetic modifications introduced by the vaccine are likely the source of these differential responses. In this paper, we present the evidence that vaccination, unlike natural infection, induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health.
We explain the mechanism by which immune cells release into the circulation large quantities of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites.
We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances are shown to have a potentially direct causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, increased tumorigenesis, and DNA damage.”
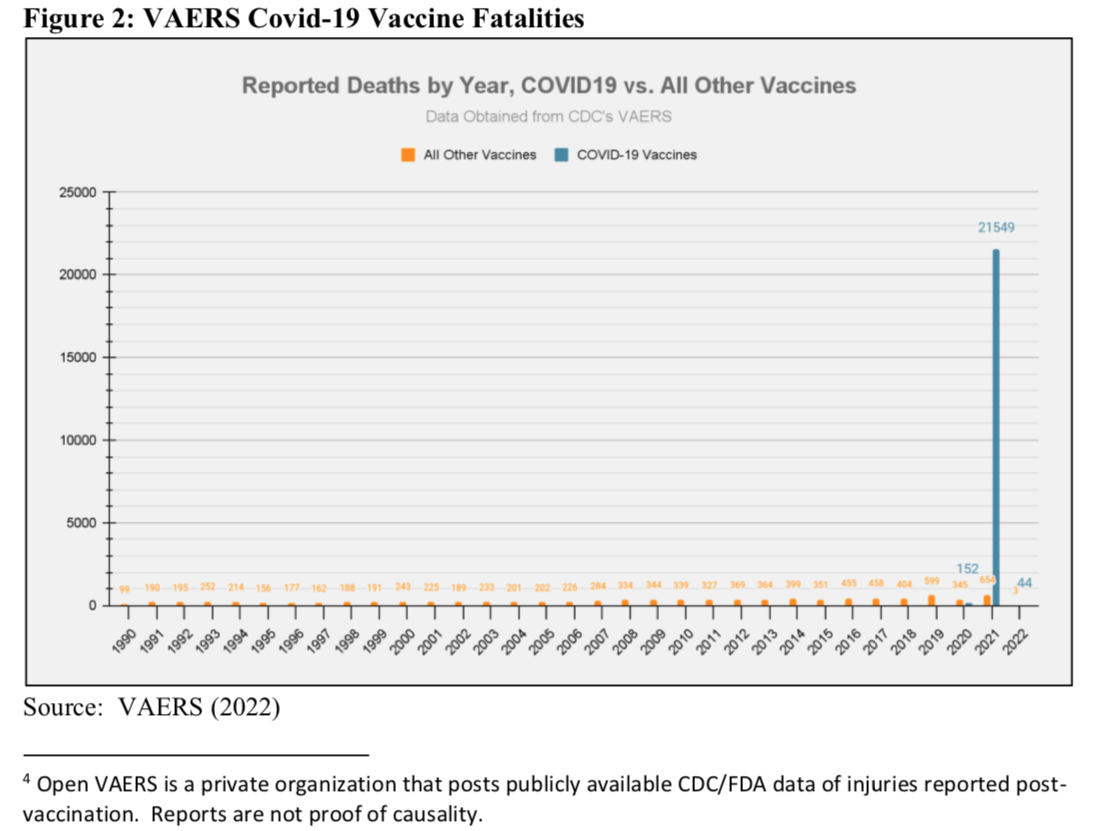
The study includes evidence from the Vaccine Adverse Event Reporting System (VAERS) to support its hypothesis. While health officials refuse to acknowledge that COVID-19 shots have caused deaths, clinically trained reviewers analyzed a sample of COVID-19 vaccine deaths reported in VAERS and found that only 14% of them were certainly not due to the vaccine.21
This means that the remaining 86% may have been related to the shots. Further, while it’s often stated that VAERS reports are made by laypeople, and therefore suggested to be unreliable, the review found that at least 67% of the COVID-19 vaccine death reports they analyzed were made by health service employees.22
Overall, McCullough and colleagues warn that COVID-19 shots subvert innate immunity, which could reduce the ability to combat future infections. Further, once damaged by the shots, the immune system may be less able to detect and prevent malignant transformation within cells.
They also suggest that exposure to spike protein-containing exosomes and mRNAs may induce an inflammatory cascade that further leads to disease. In concluding that COVID-19 shots are not positive contributors to public health, the study notes:23
“In the end, we are not exaggerating to say that billions of lives are at stake. We call on the public health institutions to demonstrate, with evidence, why the issues discussed in this paper are not relevant to public health, or to acknowledge that they are and to act accordingly.
Until our public health institutions do what is right in this regard, we encourage all individuals to make their own health care decisions with this information as a contributing factor in those decisions.”
Can You Lessen the Potential Damage?
Those considering COVID-19 shots must carefully weigh the evidence of risks before making a decision. But if you’ve already been injected and want to reduce your risk of any potential complications, there are a few basic strategies I recommend:
Measure your vitamin D level and take enough vitamin D orally (typically about 8,000 units/day for most adults) and/or get sensible sun exposure to make sure your level is 60 to 80 ng/ml (150 to 2000 nmol/l).
Eliminate all vegetable (seed) oils in your diet, which involves eliminating nearly all processed foods and most meals in restaurants unless you can be sure the chef is cooking only with butter. Avoid any sauces or salad dressings in restaurants, as they are loaded with seed oils. Also avoid chicken and pork, as they are rich in linoleic acid, the omega-6 fat that nearly everyone consumes far too much of and contributes to oxidative stress.
Consider taking around 500 milligrams a day of NAC, as it helps prevent blood clots and is a precursor for your body to produce the important antioxidant glutathione.
Consider taking fibrinolytic enzymes, which digest the fibrin that leads to blood clots, strokes and pulmonary embolisms. The dose is typically two, twice a day, but must be taken on an empty stomach, either an hour before or two hours after a meal. Otherwise, the enzymes will digest your food and not the fibrin in the blood clot.