Dr. Mercola Estimates that More Adults and Kids Have Died From COVID Injections than the Virus based on CDC's Acknowledgment that VAERS Undercounts the Number of Vax Deaths (reporting only 1%)
/STORY AT-A-GLANCE
One team published an engineering analysis to determine the current underreporting factor (URF) from the VAERS information and found the factor to be 41. When applied against the government data they found 173% more children died from the vaccine than from the illness
Using this same URF, the number of deaths from COVID rose to 815,326 and the number permanently disabled to 1,338,404. To date, the total reported deaths from the infection is 803,043, which means the shot has killed more children and adults than the virus
Although there is little reason to give children the shot, officials are spinning the idea that it is needed for herd immunity. Yet, health officials must be aware there is a significant lack of evidence to support this, and children are dying in the process
Pilot deaths and injuries affect commercial flights, logistical distribution of goods and military readiness. In one affidavit as part of a federal lawsuit against the military vaccine mandate, physician Lt. Col. Theresa Long alleges protocols are not followed after the COVID shot

From [Mercola] and [HERE] Many scientists and health experts have warned that vaccinating children against COVID-19 is unnecessary and extremely risky. Since the beginning of the pandemic, it has been obvious that children were at exceptionally low risk for hospitalization and death from the infection.1 Despite this, massive efforts are underway to ensure that every child gets a shot.
If the current data from the Vaccine Adverse Events Reporting System (VAERS)2 are any indication of what the future holds, we are facing the greatest public health calamity in modern history. I believe it is not a new COVID-19 variant causing this, but the current vaccination campaign. Unfortunately, I have no doubt that the deaths caused by the vaccines will end up far exceeding the number of deaths from the illness.
Despite the clear and present dangers of this genetic therapy, vaccine makers, encouraged and endorsed by government health agencies, are steamrolling ahead with trials and recommendations for the shot in children. In May 2021 parents found out that their children can get vaccinated without their consent if they fall under something called the “mature minor” doctrine. 3
This allows providers to treat minors, without parental consent, under certain circumstances. The age group under question was between ages 14 and 18 when there is a “rebuttable presumption of capacity, and the physician may treat without parental consent unless the physician believes that the minor is not sufficiently mature to make his or her own health care decisions.”
In July, two lawsuits were filed in federal court that challenged the Washington D.C. city law which allowed minors to be vaccinated without parental consent.4 In September 2021, The Guardian reported that children aged 12 to 15 in the U.K. may be administered a COVID-19 shot by teams in the school system without parental consent.5
If parents do not consent but the child wants the vaccine, the team can determine if a 12-year-old is able to make an informed decision. Most recently, one California mother spoke to the news media and expressed outrage after the school system allegedly offered her son a pizza in exchange for his taking the genetic therapy shot.6
With each passing month, it becomes more obvious that the battleground in the fight for liberty and freedom has been taken to our young children. A recent review of data7 from the CDC and the Vaccine Adverse Event Reporting System (VAERS) shows that more children have died from the vaccine than have died from the illness.
VAERS Underreporting Factor Affects Data
To compare the number of deaths from COVID illness against those who have died from the genetic therapy injection, we must address the known underreporting factor in VAERS. To date, the VAERS database is the only reporting system used by the CDC and FDA that is accessible to the public. According to VAERS, it:8
“… is a passive reporting system, meaning it relies on individuals to send in reports of their experiences. Anyone can submit a report to VAERS, including parents and patients.”
Additionally, it is the only area where the public, including doctors and other medical professionals, can voluntarily report vaccine adverse events, including death. According to VAERS,9 health care professionals are mandated by law to report serious injury adverse events that occur within a specified time period after the shot, and those events that are listed by the manufacturer as a contraindication to further doses.
However, the system only “encourages” providers to report events after vaccination whether the shot caused the event or not. In other words, the system depends on the health care professionals' knowledge that the VAERS system exists and their willingness to spend time filling out the document which asks for:10
While much of this information is necessary for data tracking, you can see how the time-consuming nature of filling out this form can easily become overwhelming when doctors have multiple patients with adverse events from the COVID-19 shots.11 Lack of knowledge of the system, and a growing physician shortage12 with subsequent lack of time have also likely contributed to the underreporting factor (URF).
In an early grant report submitted by the U.S. Department of Health and Human Services, which is part of the VAERS system, the writers admitted that:13
“Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.”
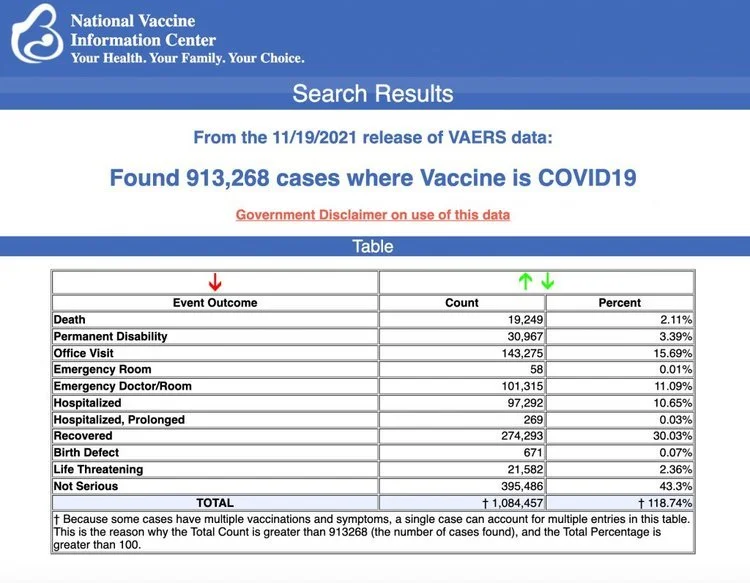
As of December 3, 2021, there were 946,461 adverse events and 19,886 deaths reported to the system.14 If only 1% of the events are reported, this translates to 94.64 million adverse events and 1.98 million deaths. To ascertain a better estimate of how many people have been injured from the current genetic injection, the issue of the URF was again addressed in a paper published in November 2021.15
The process for defining a new URF was published in a 62-page paper.16 Using an engineering analysis of the available data and judgment based on peer reviewed literature and expertise of the scientists, an underreporting factor of 41 was determined.
Agency Data Show 173% More Children Died From Shot Than Virus
In this short video, you’ll hear just several of the stories of parents who are grieving the loss of their children after giving them a vaccine they were promised would protect them. Many, thinking they were doing the right thing, took an experimental shot and have left devastated parents and families behind.
While evaluating the data, one of the writers of the paper, Steve Kirsch, recognized the gravity of the situation as it relates to the number of children who have died after taking the vaccine versus the number who have died from the illness. CDC data ending December 8, 2021,17 shows 757 children younger than 18 were listed as casualties of COVID-19.
He points out that many of these deaths, like those in adults, are likely children who died with COVID and not from COVID.18 However, to maintain simplicity, he used those numbers for comparison. Then, using data from VAERS ending December 3, 2021, he found 32 deaths from the vaccine.
Using the URF of 41, this suggests there have been 1,312 deaths that are likely to have been caused by the injection as compared to the 757 deaths the CDC records as having been caused by the illness. If you do the math, this means the shot has killed roughly 173% more children than the illness.
Using the same URF of 41 and the current data ending December 3, 2021, from OpenVAERS we can estimate there should have been 38,804,901 reports and 815,326 deaths caused by the injection. This is vitally important as the total number of deaths recorded for COVID-19 as of December 15, 2021. is 795,839.19 This means the shot has currently killed more children and adults than the virus.
Pilot Deaths, Injuries and Shot Mandates Affect Shortage
Pilot deaths and injuries affect commercial flights, logistical distribution of goods and military readiness. In mid-2020, thousands of pilots were laid off or decided to retire when flights were canceled around the country and around the world during lockdowns. Government mandates for the genetic therapy shot have also curbed the hiring of potential aviators.21
It takes up to two years to train a pilot, and Boeing estimates there will be a need for more than 600,000 new pilots over the next two decades. After the release of the shot in 2021, some noted an excessive number of pilot deaths in 2021, versus the number who died in 2019 and 2020.22
As the data on this situation continue to be released, it’s important to note that one Army flight surgeon has also stepped forward to warn that the COVID jab may increase the risk of sudden cardiac death among military pilots.23
Physician Lt. Col. Theresa Long filed an affidavit alleging the Army isn’t following DOD protocols to screen for side effects of myocarditis associated with the Pfizer and Moderna shots. The affidavit is part of a federal lawsuit against the vaccine mandate for the U.S. military. In the affidavit Long claims:24
“… there is no functional myocardial screening currently being conducted … it is my professional opinion that substantial foreseen risks currently exist, which require proper screening of all flight crews. Based on the DOD’s own protocols and studies, the only two valuable methodologies to adequately assess this risk are through MRI imaging or cardio biopsy which must be carried-out.”
In October 2021, The Defender,25 the publication of the Children’s Health Defense, asked a question that many may have overlooked. Are these vaccine mandates that appear to be reducing critical services and personnel, such as pilots, health care providers and first responders, an intentional sabotage designed to weaken America and expand control?
The loss of critical pilots is not only the result of death, but also life-altering disabilities after the shot. The Defender26 covered Sen. Ron Johnson’s, R-Wis., expert panel on COVID vaccine injuries, during which a 33-year-old commercial airline pilot from Cleveland, Mississippi, testified about his injuries.
Cody Flint had been healthy with no underlying medical conditions before receiving Pfizer’s genetic therapy injection. His first dose was February 1, 2021. Within 30 minutes he developed a severe headache that evolved into a burning sensation in his neck. Two days later he realized something wasn’t right, but only after having taken his airplane into the air. He described what happened next:27
“I was starting to develop tunnel vision and my headache was getting worse. Approximately two hours into my flying I pulled my airplane up to turn around and felt an extreme burst of pressure in my ears. Instantly I was nearly blacked out, dizzy, disoriented, nauseous and shaking uncontrollably. By the grace of God, I was able to land my plane without incident, though I do not remember doing this.”
The doctors initially told him he had an attack of vertigo and a severe panic attack. However, without a history of either, and a continuing decline of his medical condition, the doctors then told him that ”only an adverse reaction to the Pfizer vaccination or major head trauma could have caused this much spontaneous damage.”
After one year and numerous spinal taps and two surgeries, Flint shared that the vaccine stole his career and his future. He spent all his savings to pay his medical bills and his family “is on the verge of losing everything we have.”
Statistical Tricks Behind Fear Mongering
It is important to note here that the claims made by Pfizer that the vaccine is 95% effective is not an effectiveness rating you may imagine. You might think that 95% effective means that the shot protects 95 out of 100 people.
But that is something called a relative risk reduction, which actually is the difference in event rates for both groups being studied.28 In other words, it’s the reflection of the number of vaccinated people who got COVID during the trials compared to the number who were not vaccinated. If you look at the absolute risk reduction, which is far more relevant for public health measures, you’ll see that number is actually less than 1%.29
This means that out of 100 people who got the injection, it is effective for less than one person. While this makes the vaccine of dubious benefit, it also speaks to the propaganda and fear-mongering vaccine makers and vaccines stakeholders have used to promote the dangerous shot — especially when the National Institutes of Health says absolute risk reduction “is the most useful way of presenting research results.”30
Experts Are Using Herd Immunity Reasoning to Convince Parents
Since children have little reason to get the COVID shot, health officials are spinning the idea that they should be vaccinated for the sake of herd immunity. They want you to believe that not only should you look at the people around you as vectors of disease, but also that children could be asymptomatic carriers and supposedly silently spreading a deadly disease to Grandma’s house.
What they aren’t telling you, and the media is not covering, are the studies that show children are not driving the pandemic, and in fact appear less likely to transmit COVID-19 than adults.31 The Children’s Health Defense noted:32
“In short, public health leaders say, parents must ‘vaccinate the young to protect the old.’ Given the federal government’s estimate that one vaccine injury results from every 39 vaccines administered, it seems clear that officials expect children to shoulder 100% of the risks of COVID vaccination in exchange for zero benefit.”
Herd immunity occurs when enough people have acquired immunity to an infectious disease so that it no longer is widely spread in the community. This is calculated using a reproductive number or R0.33 This is the estimated number of new infections that may occur from one infected person. R1 means that one person who is infected is expected to infect one other person.
When R0 is below 1 it indicates that cases are declining and R0 above 1 suggests that they are on the rise. While it’s far from an exact science, a person’s susceptibility to infection is known to vary depending on factors including age, health and contacts within the community.
The initial calculation for COVID-19 health intervention tracking was based on assumptions that each person had the same susceptibility and would mix randomly with others in the community. However, a study published in Nature Reviews Immunology34 suggested the herd immunity threshold for COVID-19 may need adjustment since children are less susceptible to the disease. The scientists wrote:35
“Another factor that may feed into a lower herd immunity threshold for COVID-19 is the role of children in viral transmission. Preliminary reports find that children, particularly those younger than 10 years, may be less susceptible and contagious than adults, in which case they may be partially omitted from the computation of herd immunity.”
In other words, the idea that we must vaccinate children to protect adults is not backed by evidence in this illness. After decades of studying vaccine research and holding responsible positions in health care, you would hope that individuals like Dr. Anthony Fauci,36 director of the National Institute of Allergy and Infectious Diseases and Dr. Rochelle Walensky,37 director of the Centers for Disease Control and Prevention, should understand the science.
If an assumption is made that these individuals do understand the science that doesn’t support vaccinating children, and they have at least glanced at the VAERS data collected by the CDC and FDA, then you must ask the question — what is the underlying goal of vaccinating children with a potentially lethal and disabling shot when they have an exceedingly low risk of severe COVID-19 or dying from the illness?
Sources and References
1, 31 Pediatrics, 2020;146(2)
7 Estimating the Number of COVID Vaccine Deaths in America, November 1, 2021
13 Health and Human Resources, Grant Final Report, Results page 6
17 Centers for Disease Control and Prevention, December 8, 2021, last table
19 Centers for Disease Control and Prevention, Daily Updates of Totals by Week and State
34, 35 Nature Reviews Immunology 2020, doi.org/0.1038/s41577-020-00451-5
37 Centers for Disease Control and Prevention, November 2, 2021